
Join us for the second annual Accuray Exchange Showcase: Conference Highlights from 2025, your opportunity to explore the impactful research and innovations using the CyberKnife® and Radixact® Systems, presented at leading global conferences, including ESTRO, RSS, ISRS, AAPM and ASTRO. Beginning February 2nd, this four-day event will feature four daily sessions, each designed to give you a comprehensive overview of cutting-edge technologies, clinical applications and emerging trends shaping the future of radiation oncology.
Each webinar is pending approval by CAMPEP (MPCEC) and ASRT (Category A credit), with credits determined by the webinar duration.

4:00 PM
Presenter: Alfredo Conti, M.D., Ph.D., FEBNS (University of Bologna, IRCCS Institute of Neurological Sciences of Bologna, Italy)
4:05 PM
Presenter: Pantaleo Romanelli, M.D. (Renaissance Institute of Stereotactic Radiosurgery and Precision Oncology, Winter Park, Florida , USA)
4:15 PM
4:25 PM
Neuroanatomical Synergy in Cyberknife Stereotactic Ablative Neuromodulation: Revisiting Contouring Paradigms with Dopamine PET-CT and Fgatir MRI for Ventral Intermediate Nucleus Targeting in Parkinson’s Disease for Improved Outcomes
4:35 PM
Hypofractionated radiosurgery for functioning and non-functioning pituitary adenomas after surgery: Our working experience with Cyberknife unit.
4:45 PM
Single center clinical experience with Cyberknife radiosurgery for skull base meningiomas
4:55 PM
Long-Term Outcomes of Vestibular Schwannoma Treated with Stereotactic Radiosurgery: A Retrospective Study from a Single Institution
Presenter: David J. Park, MD, Ph.D., FCNS (Stanford University School of Medicine · Palo alto, USA)
5:05 PM
Multi-sequential stereotactic radiosurgery (SRS) for brain metastases: 10-year experience from the CHUV (Lausanne, Switzerland) brain metastasis clinic.
Presenter: Luis Schiappacasse, M.D. (CHUV, Lausanne, Switzerland)
5:15 PM
Treatment of glomus tumor with CyberKnife.
Presenter: Zeno Perini (San Bortolo Hospital, Vicenza, Italy)

4:00 PM
Welcome
Presenter: Asal Rahimi, M.D., MS, (U.T. Southwestern Medical Center, Dallas, TX, USA)
4:05 PM
Stereotactic Radiotherapy Boost in Locally Advanced Cervical Carcinoma Patients (STARBACS): Up-to-Date Results of a Phase II, Single Arm, Monoinstitutional Study
Presenter: Giacomo Ferrantelli, M.D. (University of Messina, Messina, Italy)
4:15 PM
Evaluation of New SGRT-Based Approach to DIBH for Left-Sided Breast Cancers on a Helical Delivery Platform
Presenter: Sanjay Hunugundmath, M.D. (Sahyadri Superspecialty Hospital, Pune, India)
4:25 PM
Automated Deep Inspiration Breath-Hold (DIBH) in Breast Radiotherapy: A Comprehensive Assessment of the VitalHold System on the Radixact Platform
Presenter: Paul RETIF, Ph.D. (CHR Metz-Thionville, Metz, France)
4:35 PM
Long-term follow-up results of helical tomotherapy for non-metastatic breast cancer: single center experience
Presenter: Abdelkarim Uakkas, M.D. (Institute Curie, Paris, France)
4:45 PM
Five-Year Outcomes of Robotic Stereotactic Accelerated Partial Breast Irradiation for Early-Stage Breast Cancer
Presenter: Rachelle Lanciano, M.D. (Crozer Keystone Healthcare System, Department of Radiation Oncology, Havertown, PA)
4:55 PM
Phase I Pre-Operative Single Fraction Dose Escalation Ablative Stereotactic Partial Breast Irradiation (S-PBI) Trial for Early-stage Breast Cancer
Presenter: Asal Rahimi, M.D., MS (U.T. Southwestern Medical Center, Dallas, TX, USA)

4:00 PM
Welcome
Presenter: Vedang Murthy, M.D., DNB, DipEPP (Tata Memorial Centre, Mumbai, India)
4:05 PM
One-day urethral-sparing, HDR-like, prostate cancer robotic SBRT: preliminary results of the PRO-FAST trial
Presenter: Andrei Fodor, M.D. (IRCCS San Raffaele Scientific Institute, Milan, Italy)
4:15 PM
A Phase I/Ib, Single Arm Study of Two Fraction SBRT with SIB for the Treatment of Localized Prostate Cancer: Early Toxicity Outcomes
Presenter: Jonathan Lischalk, M.D. (Georgetown University Hospital, Washington, D.C., USA)
4:25 PM
To Space or Not to Space: The EPIC question for Prostate Stereotactic Radiation (SBRT) with or without Hydrogel Rectal Spacer (RS)
Presenter: Madeline Flanagan (Dan L. Duncan Comprehensive Cancer Center, Baylor College of Medicine, Houston, TX, USA)
4:35 PM
Frameless Robotic Radiosurgery System Stereotactic Body Radiation Therapy (SBRT) Dose Escalation Prostate Cancer Trial (CK-DESPOT) for Unfavorable Intermediate and High-Risk Prostate Cancer
Presenter: Rachelle Lanciano, M.D. (Crozer Keystone Healthcare System, Department of Radiation Oncology, Havertown, PA, USA)
4:45 PM
Two-Year Toxicity Outcomes from Pace-C: Stereotactic Body Radiotherapy (SBRT) Versus Moderate Hypofractionated Radiotherapy (MHRT)
Presenter: Ragu Ratnakumaran, M.D. (The Royal Marsden NHS Foundation Trust, London, United Kingdom)
4:55 PM
Bladder Adjuvant Radiotherapy (BART): Clinical Outcomes from a Phase III Multicenter Randomized Controlled Trial
Presenter: Vedang Murthy, M.D., DNB, DipEPP (Tata Memorial Centre, Mumbai, India)

4:00 PM
Welcome
Presenter: Barbara Alicja Jereczek-Fossa, M.D., Ph.D. (European Institute of Oncology, Milan, Italy)
4:05 PM
A review of 130 Cyberknife spinal metastasis SABR treatments at one centre to assess risk of spinal cord toxicity
Presenter: Timothy Jackson (Queen Elizabeth Hospital, Birmingham, United Kingdom)
4:15 PM
Efficacy and Safety of Donut-Shaped Circumferential Spine CyberKnife Stereotactic Body Radiotherapy for Metastatic Spine Disease
Presenter: David J. Park, MD, PhD, FCNS (Stanford University School of Medicine, Palo Alto, USA)
4:25 PM
Stereotactic Body Radiotherapy (SBRT) Boost Following Urgent 3D Conformal Radiotherapy in the Treatment of Metastatic Epidural Spinal Cord Compression (MESCC): A Phase I Feasibility Trial
Presenter: Elysia Donovan, M.D. (McMaster University – Juravinski Cancer Centre, Hamilton, ON, Canada)
4:35 PM
Use of Stereotactic Body Radiotherapy (SBRT) for Spine Metastases with Robotic Radiosurgery Unit Cyberknife in Patients with Oligometastatic Disease
Presenter: Eva Fernandez Lizarbe, M.D. (H. U. Ramón y Cajal, Madrid, Spain)
4:45 PM
Increased iso-toxic dose to the target in oligometastatic abdominal lymph nodes using CT-guided online adaptive SBRT
Presenter: Lucy A. van Werkhoven, M.D. (Erasmus MC Cancer Institute, University Medical Center, Rotterdam, Netherlands)
4:55 PM
Stereotactic Body Radiotherapy for the Treatment of Oligometastases Located in the Peritoneum or in the Abdominal Wall: Preliminary Results from a Mono-Institutional Analysis
Presenter: Francesco Cuccia, M.D. (ARNAS Civico Hospital, Palermo, Italy)
5:05 PM
Higher disease-free survival observed for complete response after SBRT in oligometastatic gynecologic tumors
Presenter: Gaia Parma, M.D. (IRCCS San Raffaele, Milan, Italy)
5:15 PM
The Changing Dogma in Oligometastatic Renal Cell Carcinoma – SBRT
Presenter: Papaiah Susheela Sridhar, M.D. (Apollo Cancer Centre, Bengaluru, India)

Name of Institution
City, State
K. E. Hoffman1, S. F. Shaitelman1, W. Qiao2, R. Z. Zacharia3, I. Y. Arzu4, E. Bloom1, C. R. Goodman1, M. M. Joyner1, L. L. Mayo5, M. P. Mitchell1, G. H. Perkins4, J. Reddy3, P. Singh6, M. C. Stauder1, E. A. Strom1, V. K. Reed1, P. J. Schlembach3, W. Tereffe4, W. A. Woodward1, and B. D. Smith1; 1Department of Breast Radiation Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX, 2Department of Biostatistics, The University of Texas MD Anderson Cancer Center, Houston, TX, 3Department of Radiation Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX, 4The University of Texas MD Anderson Cancer Center, Houston, TX, 5Department of Radiation Oncology, Division of Radiation Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX, 6Department of Breast Surgical Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX
Purpose/Objective(s): Although RNI improves breast cancer survival, it increases risk of upper extremity lymphedema. We hypothesized that hypofractionated RNI may reduce lymphedema risk.
Methods: Patients with a recommendation for RNI for cT0-T3, N0-N2a, N3a invasive breast cancer were randomized between standard RNI (STD-RNI: 50 Gy to breast/chest wall and 45 Gy to RN) or shorter RNI (SH-RNI: 40.05 Gy to breast/chest wall and 37.5 Gy to RN). Patients were stratified by receipt of chemotherapy, body mass index (BMI), type of axillary surgery, and difference in arm volume prior to RNI. RN targets included the internal mammary, infraclavicular, and supraclavicular nodal basins; the level I and II axilla was treated if axillary lymph node dissection was not performed. Boost to the tumor bed or chest wall was permitted. Lymphedema was assessed via standard toxicity grading by the treating physician and by serial perometry measurement prior to surgery, post-operatively and then 6, 12, 18, and 24 months after radiation. The primary outcome was defined as a =10% relative difference in arm volume on at least one post-radiation perometry assessment, normalized by the pre-operative perometry measurement. Secondary outcomes included comparison of physician-reported toxicities using the NCI CTCAE v4.0 scale graded weekly during RT, at 6 months, and then annually. Fisher’s exact tests compared groups. Local-regional recurrence (LRR) was calculated using the Kaplan-Meier method and compared using the log-rank test.
Results: 324 patients across 5 treatment centers were enrolled and randomized from 2017 to 2022 with median follow up of 4.75 years. Clinical-pathologic covariates were well-balanced by treatment arm. Median age was 54 years, 64% were Non-Hispanic White, and 39% had BMI >30. 57% underwent mastectomy with or without reconstruction and 42% underwent segmental mastectomy. 68% underwent axillary lymph node dissection and 90% received chemotherapy. Perometry-assessed lymphedema, the primary outcome, was less common after SH-RNI (29%) than STD-RNI (36%), but the difference was not statistically significant (p=0.24). In contrast, physician-assessed lymphedema was significantly less common with SH-RNI than STD-RNI (15% vs. 27%, p=0.009). Patients randomized to SH-RNI were less likely to experience any grade =2 toxicity (52% vs. 78%, p<0.001). Pneumonitis was uncommon and similar between groups (3% vs 2%, p=0.46). There were no brachial plexopathy events. Five-year LRR risk was 3% with SH-RNI and 2% with STD-RNI (P=0.48).
Conclusion: In this primary outcome analysis of a multisite phase III randomized clinical trial, SH-RNI did not lower risk of perometry-assessed lymphedema. However, SH-RNI conferred a low risk of LRR and reduced the risk of physician-reported lymphedema and grade 2 or higher toxicity when compared to STD-RNI.

Renaissance Institute of Stereotactic Radiosurgery and Precision Oncology
Winter Park, Florida , USA
Pantaleo Romanelli1, Giancarlo Beltramo2, Evan Thomas3, Alfredo Conti4
1. Neurosurgery, Renaissance Institute of Stereotactic Radiosurgery and Precision Oncology, Winter Park, Florida , USA 2. Radiation Oncology, CDI, Milano, ITA 3. Radiation Oncology, Ohio State University, Columbus, USA, 4. Neurosurgery, University of Bologna, Bologna, ITA
Objectives:
Trigeminal Neuralgia (TN) is a devastating pain disorder often affecting elderly patients. Medical therapy failure is common, either due to drug intolerance or refractoriness. Surgical treatment options in very old patients can be restricted by a variety of health issues. Frameless radiosurgery provides the least invasive treatment today available for TN. Radiosurgery is a widely proven treatment for TN with an exceedingly rare complication rate (aside from sensory dysfunction). This paper aims to investigate the safety and efficacy of frameless radiosurgery for TN in the elderly population.
Methods:
A cohort of 503 TN patients treated with frameless Cyberknife radiosurgery from 2013 to 2023 was retrospectively analyzed to extract outcome data regarding patients older than 80 years. Pain intensity was assessed using the Barrow Neurological Institute Pain Scale (BNI-PS) and the Visual Analogue Score (VAS). Facial numbness was evaluated using the BNI Numbness Scale (BNI-NS). Pre- and post-treatment scores have been assessed, respectively, immediately before undergoing treatment and 3,6,9 and 12 months after. The post-treatment scores after 12 months are reported. Treatment protocol has been previously described: in short, a 6 mm segment of the nerve in retrogasserian/midcisternal location typically receives a prescribed dose of 60 Gy. Prescription isodose is usually set at the 80%. Maximum dose does not exceed 75 Gy. Treatment volume is typically around 30 mm³. In case of retreatment due to failure of the first treatment or relapse, the dose typically prescribed is 40 Gy. Treatment is tailored to patient anatomy, so that length of the nerve treated, prescribed dose and prescription isodose, maximum dose and treatment volume may change substantially from case to case.
Results:
This cohort of 503 patients included 298 patients younger than 70-year-old (59%) and 205 patients older than 70 (41%). Patients older than 70 included 134 patients aged 70-79 (27%), 62 patients aged 80-89 (12%) and 9 patients aged 90-100 (2%). Clinical outcomes of 71 patients aged 80 to 100 years (14 % of the entire cohort, median age 83 y) are reported. The median age of the 90–100-year-old group was 92 y. The median age of the 80–89-year-old group was 82 y. The median prescribed dose in both groups was 60 Gy (range 40-65 Gy). 5 patients out of 71(7%) underwent retreatment after previous CK radiosurgery receiving 45 Gy (2) or 40 Gy (3), all achieved stable pain control.
BNI-PS pre-treatment score was V in 39 patients, IV in 25, III in 7, II and I in 0. No patients had post-treatment BNI-PS scores of V and IV. Scores of III, II, and I have been found, respectively, in 9, 27 and 35 patients.
Pre-treatment VAS score was 7-10 in 64 patients, 4-6 in 7 and < 4 in 0. Post-treatment VAS score was 7-10 in 0, 4-6 in 12 and < 4 in 59.
BNI-NS pre-treatment score was one in 62 patients, II in 9, III and IV in 0. BNI-NS post-treatment score was one in 54, 15 in 9, III in 2 and IV in 0.
In summary, pain disappeared or improved in respectively 59 (83%) and 5 (7%) patients while only 2 out of 71 (3%) developed hypoesthesia associated with bothering paresthesias (grade III BNI-NS).
Conclusion:
Frameless radiosurgery provides excellent outcomes in the treatment of TN in the elderly population. No major medical or neurological complications were found. Pain improved or disappeared in 90% of the patients while only 3% developed bothering paresthesias. These data not only show remarkable efficacy and safety of frameless TN radiosurgery in the elderly population but also support the notion that radiosurgery should be considered as the elective treatment for elderly patients with medically refractory TN. Further study is needed.

Apollo Cancer Institute, Chennai, India
V. Shankar1, D. Arjundas2, S. Ghosh3, G. Laksmipathy4, S. Meenakshi Sundaram5, S. Cholayil1, V. L. Arulselvan6, S. Muthukani7, V. R. Anand8, K. Bhanu9, and V. Sai Shreya10
1Apollo Cancer Centers, Chennai, India, 2Chief Neurologist, Mercury Hospital, Chennai, India, 3Dept. of Neurosurgery, Apollo Proton Cancer Center, Chennai, India, 4Dept. of Neurology, Apollo Hospitals, Greams Unit, Chennai, India, 5Apollo Hospitals, Madurai, India, 6Dept.of Neurology, Apollo Hospitals, Greams Unit, Chennai, India, 7Dept. of Neurology, Apollo Hospitals, Greams Road, Chennai, India, 8Sai Neuro Hospital, Chennai, India, 9Mehtas Hospital,, Chennai, India, 10ACSR Govt. Medical College, Nellore, India
Purpose/Objective(s):
Bilateral trigeminal neuralgia (BTN), a rare condition that poses a unique therapeutic challenge as aggressive interventions risk bilateral complications which impair QOL like facial numbness and corneal anesthesia, This study aims to evaluate the efficacy and safety of staged radiosurgery (SRS) for BTN, with a focus on adaptive dosing strategies to balance pain control and toxicity reduction.
Materials/Methods:
A retrospective cohort analysis (between 2010-2023) was conducted on 12 patients with medically refractory BTN treated using a frameless robotic radiosurgery. Patients were stratified into two cohorts: idiopathic TN (n=7) and MS-associated TN (n=5). Treatment was delivered in two stages, separated by a minimum 6-month interval to allow toxicity assessment from the first procedure. The initial SRS targeted the trigeminal nerve root entry zone (REZ) at a median dose of 85 Gy (range: 80–90 Gy) prescribed to the 50% isodose line. For the second-side treatment, doses were adapted based on post-first-SRS toxicity: patients with minimal facial numbness (BNI grade =III) received 80 Gy (n=4), while those with significant numbness (BNI grade IV) received reduced doses of 70–75 Gy (n=8). Outcomes were assessed using BNI pain intensity scale and facial numbness scale. Toxicity included bothersome numbness (BNI IV) or severe complications (e.g., anesthesia dolorosa). Non-parametric statistical analyses were employed due to small sample size, with significance set at p<0.05.
Results:
Initial pain relief (BNI I–IIIb) was achieved in 71.4% (10/14) after the first RS and 57.1% (8/14) after the second. At 2 years, 57.1% (8/14) maintained adequate control (BNI I–IIIa). Recurrence occurred in 42.9% (6/14), with a median time to recurrence of 14 months (first-treated side) and 18 months (second-treated side). Patients with MS had lower success rates (40% vs. 66.7% in idiopathic TN; p=0.29) and earlier recurrence (median: 11 vs. 16 months). Facial numbness (BNI IV) developed in 21.4% (3/14) after the first RS and 28.6% (4/14) after the second; one patient (7.1%) experienced bilateral mild numbness. No severe complications (e.g., anesthesia dolorosa, motor deficits) occurred. Higher radiation doses (=80 Gy) correlated with better pain control (p=0.04) but increased numbness risk (p=0.07).
Conclusion:
Staged radiosurgery, with a minimum time interval of 6mo, provides effective pain relief for BTN, with careful dose adaptation playing a critical role in mitigating bilateral toxicity. Reducing the second-side dose to 70–75 Gy in patients with first-side numbness significantly lowers the risk of facial sensory complications without compromising pain control. Patients with MS exhibit lower response rates, necessitating further investigation into alternative strategies. These findings highlight the importance of individualized dosing to optimize therapeutic outcomes in BTN, though larger studies are needed to refine dosing and timing protocols.

G. Lohith1, K. Sekar2, S. S. Shivalingappa3, K. Kallur3, A. K. BS3, A. Pichandi4, and H. G. ramesh Gowda5
1Immuno-Rad Lab, HCG Hospitals, BANGALORE, India, 2HCG Hospitals, Bengaluru, karnataka, India, 3Health Care Global Enterprises Ltd, Bangalore, India, 4HCG Hospital, Banglore, India, 5HCG Hospitals, Bengaluru, Karnataka, India
Purpose/Objective(s):
A frameless robotic radiosurgery system is a non-invasive approach for alleviating motor symptoms in Parkinson’s disease (PD) by targeting dysfunctional neural circuits, such as the ventral intermediate nucleus (ViM), subthalamic nucleus or globus pallidus. This system delivers highly focused radiation for precise neuromodulation. Advanced imaging, including dopamine PET-CT and fast gray matter T1-weighted MRI, enhances treatment precision. Dopamine PET-CT maps dopamine deficiency, a hallmark of PD, while fast gray matter T1 MRI improves structural visualization for accurate ViM localization. Fusing these modalities ensures precise targeting while minimal damage to healthy tissue and improving outcomes.
Materials/Methods:
9 Indian patients with tremor-predominant PD underwent CR ViM targeting using dopamine PET-CT and FGATIR MRI. The mid-commissural line served as reference, with a target 12 mm lateral to this line. A 3 mm volume was contoured above the target across three MRI slices for lesioning precision. The ViM’s horizontal extent ranged from 9 to 11 mm, necessitating individualized adjustments. Instead of relying solely on fixed measurements, we used the internal capsule as lateral endpoint, verified with FGATIR MRI. Dopamine PET-CT also aided in lateralizing the side of dopaminergic deficiency, enhancing targeting accuracy. CR provided frameless, stereotactic Vim ablation using 85Gray single fraction keeping internal capsule max dose < 35 Gray for optimal tremor control.
Results:
90% of patients experienced more than 80% tremor relief, while remaining 10% saw over 50% improvement. The multimodal imaging approach significantly enhanced Vim localization, optimizing stereotactic interventions. Internal capsule-based lateral boundary assessment improved tremor control outcomes, reducing inaccuracies seen with conventional techniques. A frameless robotic radiosurgery system proved to be non-invasive, effective alternative to traditional interventions, achieving durable tremor suppression. Statistical analysis confirms that a frameless robotic radiosurgery system significantly improves tremor severity, validating its efficacy for treating tremor-predominant Parkinson’s disease.
Conclusion:
Integrating PET-CT and FGATIR MRI enables precise ViM localization, particularly in Indian patients with anatomical variations. Using the internal capsule as a lateral boundary improves stereotactic accuracy, minimizing reliance on predefined measurements. Dopamine PET-CT further aids in lateralizing dopaminergic deficiency, supporting patient selection and intervention planning. A frameless robotic radiosurgery system offers a precise and effective non-invasive treatment option, reducing risks associated with invasive procedures
Statistic | Value |
Sample Size (n) | 9 |
Mean Pre-Treatment Grade | 3.89 |
Mean Post-Treatment Grade | 1.11 |
Mean Difference (Pre – Post) | 2.78 |
Standard Deviation of Differences | 0.83 |
t-Statistic | 10.00 |
p-Value | 8.49 × 10?6 |

Radiation Oncology, Ramón y Cajal University Hospital, Madrid, Spain
Julen Azcona Martin1, Marta Camacho Manzanares1, Eva Fernández Lizarbe1, Ignacio Maria Gómez Paloma1, Mercedes Martín Sánchez1, David Sevillano Martínez2, Juan David García Fuentes2, Adrian Durango1, María Dolores Espinosa1, Isabel Alvira1, Margarita Martín2, Patricia Martín Nieto1, Marina Alarza Cano1, Rubén Chillida Rey2, Sonsoles Sancho García1
1 2 Radiation Oncology, Ramón y Cajal University Hospital, Madrid, Spain. Radiophysicis, Ramón y Cajal University Hospital, Madrid, Spain
Purpose/Objective:
The aim of this report is to evaluate and present the clinical outcomes and tolerance profile of hypofractionated radiosurgery for both functioning and non-functioning pituitary adenomas after partial resection. The original single fraction radiosurgery has been limited to those cases presenting small and far from the organs at risk lesions. Using the new intrafraction image guided and frameless technologies, as the Robotic Radiosurgery Unit Cyberknife, we are now allowed to deliver radiosurgery in 3-5 fractions for more complex cases.
Material/Methods:
Between June 2020 and June 2024, a total of 30 patients (13 women and 17 men) with a median age of 48,5 years were treated post-surgically with radiotherapy in our center. 27 patients presented macroadenomas and only 3 microadenomas; 13 were intrasellar (43,3%), 14 presented cavernous sinus invasion (46,7%) and 3 extrasellar (10%).
7 of them were functioning adenomas (2 ACTH-secreting, 2 prolactinoma and 3 GH-secreting). Radiotherapy indications after surgery were either remanent tumor growing, biochemical failure or poor systemic treatment tolerance
A non-contrasted CT scan and a magnetic resonance (MRI) with T1, T2 and T1 with contrast and fat suppressing sequences were used in every patient for treatment planning.
Results:
The most commonly used fractionations were 24 Gy in 3 fractions and 25 Gy in 5 fractions; both used in 9 cases. For the 24 Gy in 3 fr we reached median max doses of 33,61 Gy in hypophysis, 13,8 Gy in optic chiasm; 8 Gy left optic nerve and 10 Gy in right optic nerve. Whereas for the 25 Gy in 5 fractions median max doses were 34,15Gy in hypophysis, 22,79 Gy in optic chiasm; 9,73 Gy left optic nerve and 24 Gy in right optic nerve. The median follow-up was 26 months (7-47 months). We have observed that 40% of the adenomas have decreased in size, and the rest have remained stable without any growth. Two out of six functioning patients have achieved biochemical control.
The tolerance of the treatment was excellent. Only in 10 patients (43,5%) acute toxicity was reported consisting of grade 1-2 transient cephalea. Not chronic toxicity was reported except for a single case of transient diplopia with no visual acuity lost, completely recovered after steroids.
Conclusion:
Hypofractionated radiosurgery for pituitary adenomas appears to be a feasible and safe option for patients with large volumes or sinus involvement. In our series, we report radiological responses or stability for all treated patients with acceptable acute toxicity.
Radiation Oncology, Ramón y Cajal University Hospital, Madrid, Spain
Mercedes MARTÍN SANCHEZ , Fernández Lizarbe EVA, Martín Martin MARGARITA, Sevillano DAVID, Garcia JUAN DAVID, Alba Perez BEATRIZ, Quintana JUAN VICENTE, Medina Diaz MONTSERRAT, Garcia FELICIANO, Sancho Garcia SONSOLES
Hospital Universitario Ramón y Cajal, Madrid, Spain
Objectives:
The aim of this retrospective study is to evaluate the efficacy in local control and tolerance of radiosurgery (single RS or hypofractionated HRS doses) for the treatment of skull base meningiomas
Material and methods:
We analysed the treatment of 30 patients diagnosed with skull base meningiomas treated with CyberKnife Radiosurgery between March 2020 and February 2024. Planning was performed using CT-plan with termoplastic inmobilization mask registered with brain nuclear magnetic resonance using T1-weighted MRI with contrast and fat saturation (useful in skull base tumors, orbital lesions, or surgical beds) and high-resolution T2-weighted MRI (useful in cisternal segments of cranial nerves, cavernous sinuses or Meckel’s cave). All contours are reviewed by a dedicated neuroradiologist. In resected or unresected grade 1 meningiomas, the GTV = PTV. In grade 2 meningiomas, a margin of 1-5 mm was applied, according to international contouring guidelines.
Results:
Out of 30 patients, 22 women and 8 men. Mean age 62 years old (39-87). Most common locations were: pontocerebellar angle (14p), cavernous sinus (6p), optic nerve (4p) and others (6p). 13 patients had undergone previous surgery. 83% (25p) received a total dose of 25-30Gy in 5 fractions, 17% (5p) single fraction (14-18Gy). Mean lesion volume 10cc .For the 5 fractions scheme: mean maximum dose (Dmax) in PTV was 46.04 Gy,, mean Dmax in visual pathway 30.67Gy, pituitary 36.69Gy and brainstem 30.50Gy. For 1 fraction scheme: mean Dmax in PTV was 20.96 Gy, mean Dmax in visual pathway 7.46Gy, pituitary 7.97 Gy and brainstem 9.84 Gy.Mean conformation index of 1.3.With a median follow-up of 24 months (3-59) for 26 p who underwent the first control RMI, 100% patients achieved radiological stability. Acute toxicity was reported in 46% of patients presenting minor grade 2 toxicity, most frequently mild transient headache and asthenia. Chronic toxicity was evaluated for 26p, 26% presented minor grade 2 headache (6), neurological deterioration (1) and tinnitus (1). No cases of stroke or cranial nerve palsy were reported. Radiologic radionecrosis occurred in 1 asymptomatic patient.
Conclusions:
Our clinical experience using Cyberknife RS or HRS for skull-base meningiomas shows that these schemes are safe, effective, and helpful for patients who are rarely candidates for complete resection.

Stanford University School of Medicine · Palo alto, USA
David J. Park1, Ahed H. Kattaa1, Juan J. Cardona1, Elaheh Shaghaghian1, Amirhossein Akhavan-Sigari1, Shagun Ravi Nasta1, Harini Voruganti1, Isabelle Lee1, Yusuke S. Hori1, Sara Emrich1, Louisa Ustrzynski1, Armine Tayag1, John R. Adler1, Steven D. Chang1
1 Neurosurgery, Stanford University School of Medicine, Palo alto, USA
Objectives:
Vestibular schwannoma (VS) is a benign tumor arising from cranial nerve VIII, commonly affecting the internal auditory canal and the cerebellopontine angle. This study evaluates the long-term efficacy and safety of stereotactic radiosurgery (SRS) using CyberKnife, a platform pioneered at Stanford, highlighting our institution’s extensive long-term experience and data.
Methods:
We retrospectively analyzed a total of 344 VS cases treated with CyberKnife SRS from 1998 to 2014. Data included patient demographics, clinicopathology, radiology, and treatment details. Statistical analyses included Chi-square tests, Mann-Whitney U tests, independent t-tests, and Kaplan-Meier analysis.
Results:
The median follow-up was 157 months, representing one of the longest follow-up periods reported. The mean age was 51.9 years, with 50.9% female patients. The median tumor size was 1.7 cm, with a median target volume of 0.94 cc. Median maximum and prescribed doses were 22.5 Gy and 18 Gy, respectively. NF2 patients received higher doses (P=0.016) and had longer follow-up (P=0.012). NF2-associated tumors more frequently presented with higher Koos grades and required additional interventions (P=0.025). CN V deficits correlated with CN VIII symptom resolution (P=0.002). Notably, smokers (P=0.001) and non-hypertensive patients (P=0.001) had higher symptom resolution rates. Local recurrence was higher in those with prior surgery (P=0.048). Remarkably, local control rates were 100% at 2 years, 98.8% at 5 years, 94.2% at 15 years, and 89.3% at 25 years. Overall survival was 100% at 10 years and remained at 97.1% at 25 years.
Conclusion(s):
Our extensive long-term data confirm that CyberKnife SRS provides sustained local control and safety for VS treatment over decades, reinforcing its role as a reliable and effective management strategy pioneered at Stanford.

CHUV, Lausanne, Switzerland

San Bortolo Hospital, Vicenza, Italy
Zeno Perini
San Bortolo Hospital, Vicenza, Italy
Introduction:
Glomus tumors, also known as paragangliomas, are benign, slow growing tumors, originating from neuroectodermal tissues. They are highly vascular lesions and arise from the capillary and precapillary blood vessels, located along the tympanic branch of glossopharyngeal nerve (Jacobson’s nerve). It occurs predominantly in women and are typically diagnosed between the fifth and sixth decade of life. Clinical aspects present as pulsatile tinnitus followed by conductive hearing loss, otalgia, and aural fullness.
Materials and Methods:
From January 2003 to December 2023, 51 patients (42 females and 10 males) affected by tympanojugular glomangioma were treated with CyberKnife at our Center. The age ranged from 32 to 85 years (m: 59.7, M: 62). The average lesion volume treated was 4457 mm3 (median: 2660 mm3) while the range: 91-29331 mm3. Four patients showed multicentric lesions. Six patients underwent 2 treatments and three underwent 3 treatments. While the maximum treatment doses delivered were between 16 and 27.5 Gy (average 21.3 Gy). The isodoses are between 75-80%. In particular, a maximum dose of 22.5 Gy was used on 18 patients (34%). As regards fractionation, the majority of patients, 34/51, underwent three fractions while 6 underwent a single session. No re-treatment was performed less than three years after the previous one. The FU has a range of 5-150 months for a total of 2796 months of observation (average: 65). 43 patients underwent FU, 7 patients did not show up for checks while one died from senectus. Radiological FU was scheduled at 6-12-18-24-30 and 36 months after treatment; 38 patients underwent checks with thin-layer contrast-enhanced MRI while the other 5 underwent high-definition contrast-enhanced CT due to no indication for MRI.
Results:
In 43 patients observed, 6 (14%) presented initial disease progression (PD). However, only one actually showed full-blown disease progression while five were re-treated. 27 patients (63%) experienced disease stabilization with a single treatment (SD) while 8/43 patients (23%) experienced disease dimensional regression (RD), 2 of which after retreatment. As regards the clinical aspect, 19 patients showed a clear regression of the initial symptoms; 8 showed new symptoms (not serious and/or debilitating) while 2 underwent progression (hearing loss and tinnitus). The remainder remained neurologically quo-ante.
Huashan Hospital, China
Yun Guan, Wei Zou, Li Pan, Enmin Wang, Yang Wang, Xin Wang
Shanghai, China
Background: Glioblastoma (GBM) is a tumor known for its highly vascular nature and limited treatment options upon disease recurrence. While Bevacizumab which target VEGF-A has gained approval for treating recurrent glioblastoma (rGBM), the multi-target tyrosine kinase inhibitor Anlotinib has the ability to directly target Vascular Endothelial Growth Factor Receptor (VEGFR), Platelet-Derived Growth Factor Receptor (PDGFR), and Fibroblast Growth Factor Receptor (FGFR). Theoretically, its anti-angiogenic effect may exceed that of Bevacizumab, and preliminary studies have shown its therapeutic efficacy in rGBM, indicating promising treatment potential. This study aims to present findings regarding the effectiveness and safety of combining Anlotinib with stereotactic radiosurgery (SRS) in treating patients with rGBM.
Methods: HSCK-002 is a prospective single-arm, single center, phase II study (ClinicalTrials.gov Identifier: NCT04197492). Patients who underwent surgery, standard radiotherapy, and temozolomide chemotherapy and were diagnosed with recurrence based on Response Assessment in Neuro-Oncology (RANO) criteria and/or biopsy were eligible for inclusion. Each patient underwent CyberKnife SRS (25Gy/5fx) in combination with oral administration of Anlotinib (12 mg, daily, days 1–14/3 weeks) until encountering disease progression or experiencing intolerable adverse effects. The primary objective was the investigator-assessed median overall survival (OS) using the RANO criteria.
Results:
Between December 2019 and July 2023, 22 patients (median age: 55 years; range: 28–70 years) were included. According to RANO criteria, 21 patients exhibited tumor response, with 6 achieving complete response, resulting in an objective response rate of 95.5%. Additionally, one patient maintained stable disease without progression. Median progression-free survival (PFS) was 9.1 months (95% CI, 7.5–24.7), with a 6-month PFS rate of 85.7% (95% CI, 71.9–100.0). Median overall survival was 19.5 months (95% CI, 10.6–46.8). Common adverse events included hand-foot skin reactions (40.9%), hypercholesterolemia (27.3%), and hypertension (22.7%). Four patients experienced grade 3 adverse events, accounting for an 18.2% incidence rate. Therapy discontinuation due to ischemic stroke (grade 3) occurred in one patient. No grade 4 events or treatment-related deaths were reported.
Conclusions: The combination of salvage SRS with Anlotinib demonstrated promising outcomes and manageable toxicity in managing recurrent GBM. Currently, a phase II randomized controlled trial, supported by the Shanghai Municipal Commission of Health, is underway. This trial aims to compare the efficacy of Anlotinib combined with radiosurgery against Bevacizumab combined with radiosurgery for the treatment of rGBM patients, further exploring this therapeutic regimen.
University of Messina, Messina, Italy
S. Parisi1, G. Ferrantelli2, A. M. Attisano2, C. Martinelli3, V. Sciacca2, E. Trifiletti2, M. Sciacca2, A. Potami4, A. Brogna5, C. Siracusa6, A. Ercoli7, G. Iati’1,8, and S. Pergolizzi1
1Radiation Oncology Unit – Department of Biomedical, Dental Sciences and Morphological and Functional Images, University of Messina, Messina, Italy, 2University of Messina, BIOMORF Department, Messina, Italy, 3Sbarro Institute for Cancer Research and Molcelular Medicine and Center of Biotechnology, College of Science and Technology, Temple University, US, Philadelphia, PA, 4Radiation Oncology Unit, University hospital “G. Martino”, Messina, Messina, Italy, 5Medical Physics Unit – Department of Biomedical, Dental Sciences and Morphological and Functional Images, University of Messina, Messina, Italy, 6University hospital “G. Martino”, Messina, Messina, Italy, 7University of Messina, Dipartimento di Patologia Umana dell’adulto e dell’età evolutiva Gaetano Barresi, Messina, Italy, 8University of Messina, Radiation Oncology Unit, Messina, Italy
Purpose/Objective(s):
To evaluate feasibility, toxicities, and clinical outcome (Local Control) in locally advanced cervical cancer (LACC) patients treated with concurrent radiation therapy and platinum-based chemotherapy followed by stereotactic body radiation therapy (SBRT) boost. The hypothesis is that it is possible to deliver a dose boost with SBRT in LACC patients who underwent chemo-radiotherapy (CT-RT).
Materials/Methods:
From March 2021 to December 2024, we evaluated all patients with a diagnosis of locally advanced cervical cancer (LACC), assigned with curative intent to platinum-based chemo-radiotherapy (CT-RT), and unsuitable to brachytherapy (i.e. implant refusal, impassable vaginal stenosis, impassable cervical canal stenosis). These patients have been submitted to Stereotactic Boost using a Robotic Arm LINAC.
Results:
51 patients with LACC (M0) have been enrolled. At the time of primary diagnosis all patients had FIGO 2009-2018 stage from IIb to IIIC. Median age was 51 years (range 32-72); 42/51 had histological diagnosis of squamous-cell carcinoma HPV-related and 9/51 had histological diagnosis of adenocarcinoma. During concurrent treatments all patients received weekly Platinum-based chemotherapy (40mg/mq) plus radiotherapy to a total dose on clinical target volume (CTV) of 45-50.4 Gy (1.8 Gy/fraction). All patients have been submitted to SBRT-boost (Gold Fiducial tracking) with a median total dose delivered of 21 Gy/3 fraction (range 12-24Gy) on gross tumor volume (GTV) after restaging with contrast-enhanced MRI and 18-FDG-PET. An isotropic margin of 2mm (PTV) on GTV has been applied. To contour we matched simulation-CT with contrast-enhanced MRI using the software for deformable imaging fusion. G1-G2 toxicities were: 62% dysuria, 50% fatigue G2, 10% anemia, 20% leukopenia, 25% thrombocytopenia, 5% diarrhea, 10% nausea and vomiting. None of the patients showed toxicities = G3. Median FU time 10 months (range 1-45 months). We observed Complete/Partial response (CR and PR, respectively) in 82.4% of the cases, with 30/51 CR (58.9%) and 12/51 (23.5%) PR. Progressive disease was reported in 13 patients (7 local progression, 1 local and systemic, 5 systemic).
Conclusion:
These preliminary results showed that SBRT boost was feasible and well tolerated with encouraging results in terms of local control. Our data seem to indicate that this kind of therapy is a valid therapeutic option in LACC patients who cannot be submitted to endocavitary brachytherapy. At the best of our knowledge this is the largest study reported in English literature using a Robotic Arm LINAC.

Sahyadri Superspecialty Hospital, Pune, India
S. Hunugundmath1, M. Deputy1, A. Nirhali1, V. Naik2, and S. Gadhve3
1Sahyadri Superspecialty Hospital, Pune, India, 2Amrita Institute of Medical Sciences, Kochi, Kerala, India, 3 Sahaydri Hospitals, Pune, India
Purpose/Objective(s):
Deep-inspiration breath-hold (DIBH) is a well-established technique for reducing cardiac morbidity and lung injury in left breast cancer treatments by moving the radiation field away from the heart by inflating the lungs. While this approach has been studied at length for C-arm linacs, there is a lack of evidence to support its utility on a helical delivery platform. We report on what we believe to be the 1st cohort of left-sided breast cancer patients to be treated via DIBH on a helical platform using a surface guided system (SGRT-h). We provide a dosimetric comparison with our clinic’s standard DIBH technique – respiration-control delivered on a C-arm linac (RC-c). Also, we evaluate patient comfort and ease of use on both systems.
Materials/Methods:
Patients who underwent left breast conservation surgery followed by breast radiotherapy and who could hold their breath for at least 20 s were considered for this procedure. 20 consecutive patients were included in the study. All patients underwent 3-day training for both SGRT-h and RC-c systems between Sept 2024 – Feb 2025 at our center. Upon completion of training, patients were provided with a questionnaire to assess their comfort and system ease of use. Simulation scans were acquired for both techniques and treatment plans were generated. The prescribed dose (DRX) was 40 Gy in 15 fractions and 95% of the target had to receive > 95% DRX. Organ at risk (OAR) constraints were followed based on RTOG guidelines. Mann-Whitney U statistical test was used, and level of significance was set at < 0.05.
Results:
All 20 patients were treated using the SGRT-h technique. The mean breathhold duration was 22 s. Target coverage goals were met for all plans and did not differ between groups. All OAR constraints were satisfied. There was a statistically significant difference in the mean heart dose (150 cGy and 275 cGy for SGRT-h and RC-c respectively, (p<0.007)) and in the heart V30 (0.4% and 5.5% for SGRT-h and RC-c respectively (p<0.03)). There was a trend towards lower mean LAD dose with SGRT-h (225 cGy compared to 275 cGy), however this failed to reach statistical significance (p<0.20). Similarly, a trend towards lower ipsilateral lung V5 and V20 was observed with SGRT-h (40.2 %and 16.3% respectively) compared to RC-c (50.4%and 21.7%), however this was not statistically significant. The questionnaire revealed that patients found the instructions for SGRT-h easier to understand and the treatment less restrictive.
Conclusion:
We reported on the 1st cohort of left-breast cancer patients treated with DIBH on a helical system using SGRT. Compared to our previous standard approach, this implementation offers superior dosimetry, with a significant reduction in both mean heart and LAD doses, a trend towards lower lung dose, and a higher level of patient satisfaction. We conclude that this novel implementation of DIBH can be adopted clinically.

CHR Metz-Thionville, Metz, France
Paul RETIF1,2, Abdourahamane DJIBO SIDIKOU1, Julien GRIBELBAUER1, Anwar AL SALAH1, Estelle PFLETSCHINGER1, Xavier MICHEL3
1 2 Medical Physics Unit, CHR Metz-Thionville, Metz, France. CRAN, CNRS, Université de Lorraine, Nancy, France. 3 Radiotherapy-Brachytherapy Department, CHR Metz-Thionville, Metz, France
Purpose/Objective:
To evaluate the performance of the VitalHold module for automated Deep Inspiration Breath-Hold (DIBH) treatment on the Radixact platform, focusing on its dosimetric accuracy and responsiveness to respiratory motion.
Material/Methods:
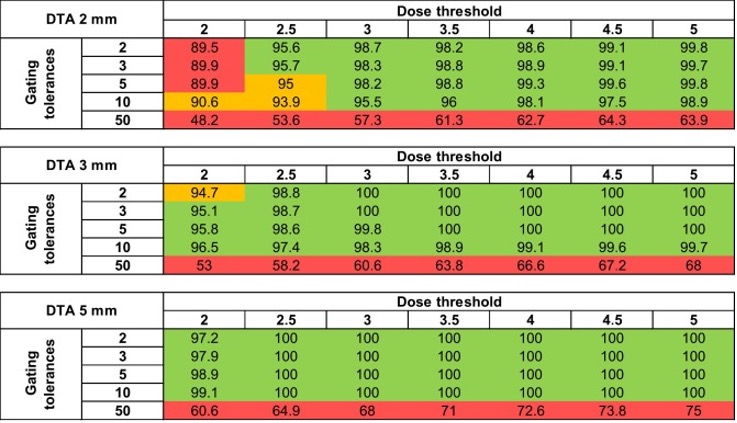
A Delta4 Phantom+ system with customized 3D-printed breast add-ons was used to simulate a clinically relevant setup for DIBH. A treatment plan was created with 40 Gy in 15 fractions using TomoDirect. The Phantom was coupled with the HexaMotion motion platform to replicate a breath-hold pattern with 2 cm amplitude and 8.84 seconds duration. The Radixact treatment unit with the VitalHold module was employed for automated beam delivery, using gating thresholds ranging from 2 to 25 mm (non-gated delivery). Respiratory motion was monitored with the Catalyst+ HD SGRT system. Dose distributions were measured with the Delta4 Phantom+ and analyzed using various gamma criteria.
Results:
The measured respiratory curve closely matched the simulated motion, with amplitude differences under 0.1 mm and cycle variations of 0.1 seconds. Minor artifacts affected gating accuracy by less than 0.7 mm. Gamma pass rates for 2 to 5 mm gating tolerances were ≥ 95%, indicating high system accuracy (Figure 1). Gating thresholds over 5 mm showed decreased but acceptable performance, while non-gated delivery yielded unacceptable gamma pass rates.
Conclusion:
The VitalHold module on the Radixact platform demonstrates strong potential for automated DIBH treatment, providing precise and reliable beam control under simulated breath-hold conditions, particularly for gating tolerances of 2 to 5 mm. This study supports the integration of automated breath-hold techniques in clinical practice.

Institute Curie, Paris, France
Abdelkarim Uakkas, Jihane Bouziane, Pierre Loap, Youlia Kirova
Radiation oncology, Institute Curie, Paris, France
Purpose/Objective:
The aim of our study is to explore the application of helical tomotherapy in the treatment of breast cancer, assessing its efficacy, safety, and role in the current therapeutic framework by analysing the clinical data and survival outcomes of our cohort of patients.
Material/Methods:
This single-center retrospective study was conducted at the department of radiation oncology of the Institute Curie (Paris, France) and included 179 patients treated with helical tomotherapy for breast cancer beetween 2009-2015.
Overall survival and progression free survival curves were plotted with Kaplan-Meier method. We also analysed the overall survival and progression-free survival data by molecular subgroups. Acute and long-term toxicity including skin, cardiac and pulmonary complications were also evaluated.
Results:
179 patients (15 of whom had bilateral cancer) were treated between 2009 and 2015 with helical tomotherapy for non-metastatic breast cancer. The median age of the patients was 53 years. Of these, 189 were treated for non specific invasive carcinoma, while 5 patients were treated for carcinoma in situ.
85.1% of patients had lymph node irradiation associated with breast or chest wall irradiation. 152 of the 163 irradiated breasts received a boost at the lumpectomy bed. The median duration of treatment was 46 days.
After a median follow-up of 10 years, there were 9 local recurrences, 2 regional lymph node recurrences and 29 patients had metastatic progression. Only 18 patients died at the end of the study, of whom 7 were cancer-related.
At 10 years, local recurrence-free survival was 95.3%, locoregional recurrence-free survival was 94.5%, metastasis free survival was 82.9%, specific survival was 94.3%, and overall survival was 88%. The occurrence of local, regional or distant recurrence correlated neither with HR or HER2 status, nor with grade, nor with the presence of emboli. In terms of molecular subgroups, recurrence-free survival was 86.3%, 90.9% and 76.7% respectively for the triple negative, HER+ and RH+/HER2- subgroups.
In terms of acute skin toxicities, 96 patients presented grade 1 radioepithelitis, 72 grade 2 and 6 grade 3. 40 patients had late skin toxicity at last follow-up. No grade 3 or higher acute or late toxicity and no radiation-induced late pulmonary or cardiac toxicity was reported.
Conclusion:
This analysis summarises the clinical data and survival results associated with helical TomoTherapy in patients with non-metastatic breast cancer, highlighting low recurrence rates and good treatment tolerance, confirming the relevance of this technique in specific indications.

Crozer Keystone Healthcare System, Department of Radiation Oncology, Havertown, PA
T. Sherman1, J. M. Cantalino2, and R. M. Lanciano3
1Drexel University College of Medicine, Philadelphia, PA, 2Department of Radiation Medicine, MedStar Georgetown University Hospital, Washington, DC, 3Crozer Keystone Healthcare System, Department of Radiation Oncology, Havertown, PA
Purpose/Objective(s):
Adjuvant accelerated partial breast irradiation (APBI) offers comparable outcomes to whole breast irradiation in select early-stage breast cancer patients. Robotic stereotactic APBI (RSAPBI) with fiducial tracking is a precise and efficient option, though long-term safety and efficacy data remain limited. This study presents 5-year outcomes from a single institution participating in a prospective registry, assessing the efficacy, safety, and tolerability of RSAPBI in women with early-stage breast cancer.
Materials/Methods:
Eligible patients were women aged =50 years with early-stage breast cancer (T1-T2, N0, M0), including histologically confirmed ER+/PR+ invasive ductal carcinoma (IDC) or ductal carcinoma in situ (DCIS). Tumors requirements were =2 cm with negative surgical margins of =2 mm. Exclusion criteria included lymph node involvement, metastatic disease, prior ipsilateral breast cancer or breast irradiation, multifocal/multicentric disease, or contraindications to radiation or fiducial placement. A robotic radiosurgery system was utilized for treatment. Four gold fiducials were implanted around the lumpectomy cavity for tumor bed delineation and tracking. CTV was defined as the cavity with a uniform 5-15 mm expansion limited to breast tissue, and PTV was CTV with 0-5 mm expansion. The prescribed dose was 30 Gy in 5 fractions. Outcomes included overall survival (OS), ipsilateral breast tumor recurrence (IBTR), toxicity (RTOG grading), and cosmetic result (Harvard Scale), assessed at 4 weeks, 3, 6, 12, 18, 24 months, and then yearly for 5 years. Kaplan-Meier curves were used for actuarial outcome analysis.
Results:
Fifty-four women (median age 66.5 years, range 51–83) were enrolled from March 2016 to May 2021. Median follow-up of the cohort is 60 months (range 0-100 months). 83.3% of women had IDC while 16.7% had DCIS. 87% were Caucasian, 9.3% African American, 1.9% Asian.
All patients received 30 Gy in 5 fractions. The median treatment duration was 9 days (range 7–14). The median CTV expansion was 10 mm (range 5-10) and PTV expansion was 3 mm (range 2-5 mm). The median PTV volume was 116 cm³ (IQR 69-156), and the median prescription isodose line was 81.5% (IQR 80-83).
There was 1 ipsilateral breast tumor occurrence with no local, regional, or distant failures. 5-year actuarial survival was 87%. No deaths were directly attributed to breast cancer. Two patients withdrew from the protocol. Grade 1 skin toxicity occurred in 5 patients (9.3%) at 1-month follow-up; no grade 2-4 toxicity was observed. Cosmetic outcomes at 5 years were rated excellent in 60% and good in 40%. Neither fat necrosis nor breast pain were reported at last follow-up.
Conclusion:
Five-year outcomes suggest that RSAPBI with fiducial tracking is a safe, effective, and well-tolerated treatment for early-stage breast cancer, demonstrating excellent local control and cosmetic outcomes.
U.T. Southwestern Medical Center, Dallas, TX, USA
A. S. Rahimi1, M. Leitch2, B. Dogan3, P. G. Alluri1, M. Arbab1, D. Li1, D. D. M. Parsons1, N. Wandrey1, D. Farr2, D. W. N. Kim4, S. Seiler3, R. Wooldridge2, N. Unni5, C. R. Nwachukwu6, I. Patel5, W. Lu7, A. Nguyen2, T. D. Chiu6, M. Stein1, E. Pina8, S. Bahrami1, H. E. Morgan9, Y. Liu10, H. L. McArthur5, S. Sahoo11, and R. D. Timmerman1
1Department of Radiation Oncology, University of Texas Southwestern Medical Center, Dallas, TX, 2Department of Surgery, University of Texas Southwestern Medical Center, Dallas, TX, 3Department of Radiology, University of Texas Southwestern Medical Center, Dallas, TX, 4Vanderbilt University Medical Center, Nashville, TN, 5University of Texas Southwestern Medical Center, Medical Oncology, Dallas, TX, 6University of Texas Southwestern Department of Radiation Oncology, Dallas, TX, 7Medical Artificial Intelligence and Automation (MAIA) Lab, Department of Radiation Oncology, UT Southwestern Medical Center, Dallas, TX, 8University of Texas Southwestern Medical Center, Dallas, TX, 9CARTI Cancer Center, Little Rock, AR, 10Department of Population and Data Sciences, University of Texas Southwestern, Dallas, TX, 11Department of Pathology, University of Texas Southwestern, Dallas, TX
Purpose/Objective(s):
Investigate pre-op single fraction SPBI dose escalation on toxicity and tumor response in early-stage HR+ breast cancer. Primary objective was escalate single fraction SPBI to an ablative dose without exceeding maximum tolerable dose(MTD). Secondary endpoints were pathologic complete response (pCR=RCB 0 or Miller Payne(MP) 5), near complete response (nCR=RCB 1 or MP 4), local control, toxicity, and cosmesis.
Materials/Methods:
Patients(pts) with <3 cm, HR+, Her2-, cN0 invasive breast cancer not requiring chemotherapy were treated on MR LINAC, robotic radiosurgery, or cobalt stereotactic breast unit with 30, 34, or 38Gy. Pts underwent endocrine therapy, and surgery post-SPBI. Median time to Surgery (MTS) was recorded.
Dose limiting toxicity (DLT) defined as grade =3 toxicity attributed to SPBI. Each cohort enrolled 7-15 pts. Dose escalation permitted if 0/7, 2/9, =3/12, or =4/15 patients experienced DLT within 90 days of SPBI. MTD exceeded if more DLTs occur in any cohort.
Results:
From 12/2019 to 5/2024, 14,15 and 15 pts were treated with median follow-up of 35,36,12.6 mo for 30,34 and 38Gy, achieving pCR+nCR rates of 64.3%, 93.3% and 93.3% respectively. For the 30Gy group, MTS post-SPBI was 5.9 mo (range 2.8-11.7) with 35.7% (5/14) achieving pCR and 64.3% (9/14) achieving pCR/nCR. MTS for 34Gy was 7.3mo(range 5.3-12): 7/15 (46.7%) had pCR while 14/15 (93.3%) had pCR/nCR. MTS for 38Gy was 11.4mo (range 8.4–12.9):10/15 (66.7%) pCR, while 14/15(93.3%) had pCR/nCR.
A time-to-surgery cutoff of 277 days best distinguished MP grade 5 (pCR), yielding an AUC of 0.765 (95% CI: 0.617 – 0.912), sensitivity 0.818, specificity 0.727. When evaluating pts who had surgery >270 days post radiation, 100%, 66.7% and 64.3% achieved pCR (p = 0.40) and 100%, 83.3%, and 92.9% achieved pCR/nCR when treated with 30Gy, 34Gy and 38Gy respectively (p = 0.69).
Tumor size >11.5mm (AUC=0.56, 95% CI: 0.37-0.74) is less likely to have a MPS of 5, but only has a sensitivity of 0.67 and +predictive value 0.58, suggesting that tumor size alone is not the best predictor of pCR. Combining MTS + size results in AUC of 0.79(95% CI:0.63-.93), with sensitivity=0.91and specificity=0.64.
Of the 15 pts with a nCR 53.3% had =3mm of residual disease. The mean ki67 was 11.0% at diagnosis and 1.8% at surgery.
There were 59 acute grade 1; 3 acute grade 2 (breast pain and dermatitis); 2 late grade 2 (breast pain and surgical washout), and 1 grade 3 (slow healing wound ulceration in a pt with uncontrolled diabetes in the 30 Gy cohort).
Conclusion:
Longer elapsed time from pre-op ablative SPBI/hormonal therapy to surgery (>9 months), leads to significantly higher pCR/nCR (>90%), suggesting potential tumor eradication with radiation/endocrine therapy alone. Incomplete biological effect are seen at earlier time points. This paves the way for possible non-surgical management for selected early-stage HR+ breast cancer pts. (NCT04040569)
30Gy | 34 Gy | 38 Gy | All Cohorts | |
nCR+pCR >270 days MTS | 5 out of 5 (100.00%) | 5 out of 6 (83.33%) | 13 out of 14 (92.9%) | 23 out of 25 (92.0%) |
U.T. Southwestern Medical Center, Dallas, TX, USA

IRCCS San Raffaele Scientific Institute, Milan, Italy
Andrei Fodor1, Laura Giannini1, Sara Broggi2, Miriam Torrisi1, Paola Mangili2, Andrea Losa3, Tommaso Maga3, Roberta Tummineri1, Chiara Lucrezia Deantoni1, Alessia Tudda2, Lucia Perna2, Roberta Castriconi2, Paolo Passoni1, Carmen Gigliotti2, Cesare Cozzarini1, Claudio Fiorino2, Franco Gaboardi3, Antonella Del Vecchio2, Nadia Gisella Di Muzio1,4
1 2 Radiation Oncology, IRCCS San Raffaele Scientific Institute, Milan, Italy. Medical Physics, IRCCS San Raffaele Scientific Institute, Milan, Italy. 3Urology, IRCCS San Raffaele Scientific Institute, Milan, Italy. 4Medicine, Vita-Salute San Raffaele, Milan, Italy
Purpose/Objective:
Several published studies have investigated the ultra-hypofractionation in single fraction for prostate cancer (PCa) (1,2,3). Here we report the preliminary results of the PRO-FAST study (NCT05936736), of one-day urethral-sparing (US), HDR-like, radical robotic stereotactic body radiotherapy (SBRT) for PCa.
Material/Methods:
The institutional ethics committee approved an interventional prospective single-arm trial of US-HDR-like SBRT for PCa patients. According to the optimal design of Simon, 13 patients will be enrolled for the first phase of the study.
The study will be interrupted if ≥2 ≥G3 toxicities are recorded within one month from the end of SBRT, otherwise the study will continue with the second phase enrolling another 52 pts for a total of 65 pts. Five additional patients will be enrolled to compensate for any drop-offs. Primary objective is acute toxicity at one month, while secondary objectives include biochemical relapse-free-, clinical relapse-free-, cancer-specific- and overall-survival, and quality of life (assessed with quality-of-life questionnaires EORTC QLQ C30 and PR25, IIEF-5, IPSS, and EPIC-26). Patients with limited disease to the prostate, assessed with prostate specific membrane antigen (PSMA) positron emission tomography/computed tomography (PET/CT) (for unfavorable intermediate (UIR) and high-risk (HR) tumors) will be included. Acceptable uroflowmetry, no previous pelvic radiotherapy and relevant comorbidities are required.
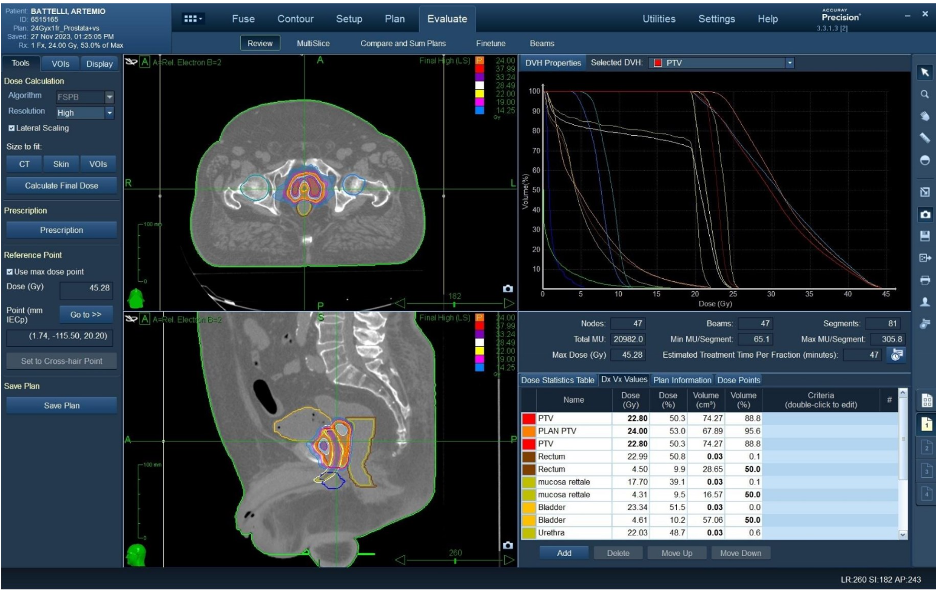
Importantly, all procedures are performed in just one day. The patient begins in the morning with the implantation of the 4 fiducials necessary for tracking, then performs in succession (with an urinary catheter inserted) the CT scan, MRI, contouring, planning, quality assurance control, and the delivery of the treatment, to a total dose of 24 Gy/1 fraction prescribed at the 50% isodose (with particular focus on sparing the urethra and rectal mucosa) (See example in Fig.1). Androgen deprivation is prescribed for 6 months for UIR and 2 years for HR patients. Short-term steroids and alpha lytics are admitted, for prophylactic purposes.
Results:
From 11/2023 to 10/2024, twelve Pca patients with a median age of 76.9 (67.2-81.2) were enrolled. Three were HR, 5 UIR, and 4 favorable intermediate risk. Median initial PSA was 8.68 (2.9-18.15) ng/ml; one patient was ISUP grade 5, two patients 4, one patient 3, and 8 patients 2. Three patients presented grade (G)2 Genito-urinary toxicity, and 7 G1. Six patients presented G1 gastro-intestinal toxicity.
Conclusion:
No G3 toxicity was recorded in the first 12 patients, so we can consider the first step of the trial as achieved; patients’ enrollment will continue.

Georgetown University Hospital, Washington, D.C., USA
J. W. Lischalk1,2, V. Santos2, B. Vizcaino3, C. Mendez4, A. Sanchez4, A. Corcoran5, S. Taneja6, D. R. Wise7, J. Divers8, A. Katz5, H. Lepor6, T. J. Carpenter4, W. Huang6, A. Tong9, M. Zelefksy10, and J. Haas4;
1Department of Radiation Medicine, Georgetown University Hospital, Washington, DC, 2Department of Radiation Oncology, Perlmutter Cancer Center at New York University Langone Hospital – Long Island, New York, NY, 3Department of Radiation Oncology, Perlmutter Cancer Center at New York University Grossman School of Medicine,, New York, NY, 4Department of Radiation Oncology, Perlmutter Cancer Center at New York University Langone Hospital – Long Island, Mineola, NY, 5Department of Urology, Perlmutter Cancer Center at New York University Langone Hospital – Long Island, Mineola, NY, 6Department of Urology, Perlmutter Cancer Center at New York University Grossman School of Medicine, New York, NY, 7Department of Medicine, Perlmutter Cancer Center at NYU Langone Medical Center, New York, NY, 8Department of Foundations of Medicine, NYU Long Island School of Medicine, Mineola, NY, 9Department of Radiology, NYU Langone Health and New York University, Grossman School of Medicine, New York, NY, 10Department of Radiation Oncology, Perlmutter Cancer Center at New York University Langone Hospital, New York, NY
Purpose/Objective(s):
Stereotactic body radiation therapy (SBRT) has been established as an effective modality for localized prostate cancer with recent level 1 evidence supporting its comparative efficacy and toxicity. Simultaneous integrated boosts (SIB) to the dominant intraprostatic lesion have demonstrated improved oncologic outcomes based on the FLAME trial. The purpose of this phase I/Ib study is to evaluate the feasibility and safety of a novel 2-fraction SBRT regimen with an MRI-guided SIB to the dominant intraprostatic lesions (PI-RADS 4+) stratified by genomic risk classification.
Materials/Methods:
This single arm, prospective study explored patients with biopsy-proven localized prostate cancer classified as low to intermediate risk per NCCN criteria. All patients underwent MRI-based SBRT treatment planning with fiducial markers and rectal spacer placement. Two fractions of SBRT were delivered to a total dose of 25 Gy in 2 weekly treatment fractions to the whole prostate with a 28 Gy SIB to the dominant lesion in patients with unfavorable intermediate risk disease or favorable intermediate risk with an elevated decipher score. Primary physician reporting grade 2+ toxicity per CTCAE version 5.0 was the primary endpoint. Follow-up was performed 30 days posttreatment and subsequently every 3 to 4 months for 2 years.
Results:
A total of 18 patients with a median age of 73 years completed treatment, with a median follow-up of 6.43 months. Prostate cancer distribution was as follows: low (n=2, 11%), favorable intermediate (n=10, 56%), and unfavorable intermediate (n=6, 33%). The decipher score distribution was as follows: low (n=8, 44%), intermediate (n=3, 17%), and high (n=7, 39%). Of the entire cohort, median prostate volume was 39.5 cc, 61% (n=11) underwent an intraprostatic micro boost with 5 patients due to an elevated decipher score, and 17% (n=3) received ADT as a component of treatment. With early follow-up, we observed only one instance of acute grade 2 GU and GI toxicity (5.5%) that occurred 9 days after treatment completion and resolved at the 1 month follow up. No instance of severe GU or GI toxicity was reported.
Conclusion:
This phase 1/1B study demonstrates that 2-fraction SBRT with or without an MRI directed SIB is a feasible and well-tolerated approach for localized prostate cancer. Toxicities with early follow-up are minimal and lower than historical controls utilizing a 2-fraction regimen. Further follow-up is required to determine the long-term efficacy and late toxicity trends. This novel fractionation regimen may offer a highly efficient and a biologically effective treatment option for selected patients, minimizing treatment burden and optimizing disease control using modern genomic stratification and advanced treatment delivery.

Dan L. Duncan Comprehensive Cancer Center, Baylor College of Medicine, Houston, TX, USA
M. M. Flanagan1, H. Mekdash1, S. P. Collins2,3, B. Collins2,3, S. Suy3, and D. A. Hamstra1
1Department of Radiation Oncology, Dan L. Duncan Comprehensive Cancer Center, Baylor College of Medicine, Houston, TX, 2Department of Radiation Oncology, Tampa General Hospital, Tampa, FL, 3Department of Radiation Oncology, University of South Florida (USF) Health Morsani College of Medicine, Tampa, FL
Purpose/Objective(s):
Following prostate RT bowel, urinary, and sexual side effects and declines in quality of life (QOL) are common. Phase 3 trials of rectal spacers using 20 or more fractions found clinical and dose benefits and less declines in QOL. However, the role of rectal spacers using SBRT is undefined.
Materials/Methods:
A prospective single institution registry of prostate SBRT between 2012-2023 was analyzed by RS use (n=290) or not (n=1815). QOL was collected via EPIC-26 at baseline, 1 mo, and serially up to 5 yrs post-RT. Treatment used CT planning with MRI fusion and 3-6 fiducials for real-time tracking with Robotic SBRT that is a frameless robotic radiosurgery system from a technology company. The CTV was the prostate plus the proximal seminal vesicles. PTV margins were 5 mm except 3 mm posteriorly. 35-36.25 Gy was delivered in 5 fractions over 1-2 weeks. No dominant nodule boost was used. Linear mixed-effects models examined the effect of time and treatment on QOL scores, accounting for within-subject variability.
Results:
There were no differences in age (69 vs 72 p=0.1), PSA (7.8 vs 7.5 p=0.3), or prostate volume (39 v 38 ml p=0.9) in those with or without RS, respectively. Use of RS was associated with more intermediate/high risk (96% v 85% p<0.001), ADT use (52% v 39% p<0.001), more Caucasian patients (63% v 55% p<0.001), and treatment more recently (p<0.001). Baseline EPIC scores were not different (Table). Declines in EPIC scores following SBRT were small with the majority approaching baseline after 6 mo and remaining stable up to 5 yrs. Mean QOL decline met pre-defined thresholds for minimally important difference (MID) only for urinary obstructive, bowel, and hormonal/vitality QOL at 1 mo and then recovered. At no time did any mean meet a threshold for 2x MID. No significant differences were observed in any QOL domain for those who received RS or not (all p>0.1). Sexual function was also not different if limited to those with baseline EPIC >60 and no ADT use (p>0.3).
Conclusion:
Robotic SBRT for definitive treatment of prostate cancer had minimal declines in QOL with stable and clinically insignificant outcomes for most domains beyond 6 mo. The use of RS did not influence QOL. The study is limited by non-randomized design, single institution, and may not apply to other RT delivery platforms. Further, baseline factors and medications may have influenced use of RS. Additional investigation through randomized controlled trials is warranted.
| Obstructive Urine | Incontinence Urine | Bowel | Sexual | Vitality Hormonal | ||||||
| SBRT | +RS | SBRT | +RS | SBRT | +RS | SBRT | +RS | SBRT | +RS | |
| BASELINE | 84.8 | 86.9 | 89.7 | 90.2 | 92.9 | 92.7 | 45.9 | 45.8 | 90.2 | 89.0 |
| Time (mo) | Change in Mean Summary Score | |||||||||
| 1 | -6.9* | -5.6* | -4.3 | -3.8 | -6.5* | -5.4* | -5.7 | -10.0* | -4.4* | -4.8* |
| 6 | +0.7 | -0.7 | -4.2 | -2.5 | -1.7 | -1.5 | -4.2 | -8.0 | -1.9 | -1.5 |
| 12 | +0.7 | -3.0 | -4.2 | -2.5 | -2.7 | -1.5 | -4.2 | -5.0 | -0.3 | -0.3 |
| 24 | +1.0 | -1.2 | -4.5 | -4.2 | -1.7 | -2.7 | -5.8 | -4.1 | +0.5 | -0.3 |
| 60 | +3.8 | -0.6 | -4.4 | -5.5 | -0.8 | 0.8 | -7.3 | -9.1 | +1.6 | +4.2* |
| MID | 5 | 6 | 4 | 10 | 4 | |||||
| *= Change meets MID; (-) = worse QOL | ||||||||||
Crozer Keystone Healthcare System, Department of Radiation Oncology, Havertown, PA, USA
M. Nguyen1, and R. M. Lanciano2
1Crozer-Chester Medical Center, Upland, PA, 2Crozer Keystone Healthcare System, Department of Radiation Oncology, Havertown, PA
Purpose/Objective(s):
Since publication of the FLAME (focal lesion ablative micro boost in prostate cancer) trial, the NCCN guidelines incorporated focal boost for intensity modulated radiation therapy. However, limited data exist on micro-boost with SBRT. This phase II clinical trial sought to assess outcomes following simultaneous integrated focal boost during a course SBRT with a frameless robotic radiosurgery system. The primary objective is to assess biochemical disease-free survival and the secondary objective is to assess severe gastrointestinal and genitourinary toxicity beyond six months of follow-up.
Materials/Methods:
Eligible patients had NCCN-defined unfavorable intermediate- or high-risk prostate cancer diagnosed within 360 days of enrollment. MRI and bone scan +/- PSMA PET/CT were required for staging. Patients received androgen deprivation therapy (ADT), and SBRT was initiated within 2 months of ADT. Space OAR gel and fiducials were required. Other inclusion criteria included prostate volume <100 cc, no prior pelvic radiation or TURP, AUA score <20, and no nodal or distant metastases. SBRT delivered 40 Gy to the prostate, with a PIRADS 4/5 nodule boost to 45-50 Gy. Proximal seminal vesicles received 36.25 Gy. Dose volume constraints were enforced for nearby at-risk organs. Toxicity was evaluated with standardized questionnaires. Biochemical control was determined by the Phoenix definition. Follow-up interval was 1, 3, 6, 12, 18, 24 months and yearly thereafter until year 5.
Results:
Thirty-three patients (median age of 66, 85% Caucasian) completed SBRT. Sixty-seven percent were stage T1c, 84.8% had a Gleason score of 7 and 57.6% were primary grade 4. Median baseline PSA was 6.5, with a median of 42% positive cores. 85% of our patients had unfavorable intermediate risk prostate cancer. The median duration of ADT was 6 months. Seventy nine percent received PI-RADS 4/5 simultaneous integrated focal boost. Median follow-up was 36 months. Toxicity was low with AUA scores peaking at 1 month (median=11, vs. baseline median AUA of 4.5) improving by three months (median=5) and stabilizing at 3-4 from 24 to 60 months. No grade 3-5 RTOG acute or late urinary or bowel toxicity was observed. Among patients with at least 24 months of follow-up (n=23), median PSA was 0 (range 0-0.6). At 36 months (n=18), 48 months (n=13), and 60 months (n=10), median PSA remained 0, with maximum PSA of 0.2, 0.09, and 0.05, respectively.
Conclusion:
This study describes a novel, safe, and low-toxicity radiation protocol for men with intermediate and high-risk prostate cancer, demonstrating that simultaneous integrated focal boost with SBRT is feasible and safe with low toxicity. Biochemical failure has not been seen in this study with 36-month median follow-up. Clinical Trial number: NCT03822494.

The Royal Marsden NHS Foundation Trust, London, United Kingdom
R. Ratnakumaran1,2, V. Hinder2, A. Chan3, S. Tolan4, P. Ostler5, H. Van Der Voet6, O. Naismith1,7, S. Jain8, A. Martin9, D. Price10, B. O’Neil11,12, A. Duffton13, J. Staffurth14, G. Sasso15,16, J. Pugh2, G. Manning2, S. Brown2, N. van As1,2, E. Hall2, and A. Tree1,2
1The Royal Marsden NHS Foundation Trust, London, United Kingdom, 2The Institute of Cancer Research, London, United Kingdom, 3University Hospitals Coventry and Warwickshire, Coventry, United Kingdom, 4The Clatterbridge Cancer Centre, Liverpool, United Kingdom, 5Mount Vernon Cancer Centre, Northwood, United Kingdom, 6The James Cook University Hospital, Middlesbrough, United Kingdom, 7Radiotherapy Trials Quality Assurance Group, London, United Kingdom, 8Queen’s University Belfast, Belfast, United Kingdom, 9Cambridge University Hospitals NHS Foundation Trust, Cambridge, United Kingdom, 10Independent Patient and Public Representative, London, United Kingdom, 11St Luke’s Radiation Oncology Network, St Lukes Hospital, Dublin, Ireland, 12Cancer Trials Ireland, Dublin, Ireland, 13The Beatson West of Scotland Cancer Centre, Glasgow, United Kingdom, 14Cardiff University, Cardiff, United Kingdom, 15Auckland City Hospital, Auckland, New Zealand, 16Faculty of Medical and Health Sciences, The University of Auckland, Auckland, New Zealand
Purpose/Objective(s):
The PACE-B trial established SBRT as a standard of care for low- and favourable intermediate-risk localised prostate cancer. PACE-C aims to demonstrate non-inferiority of SBRT compared to MHRT in intermediate- or high-risk localised prostate cancer patients receiving androgen deprivation therapy (ADT). Here, we present late toxicity outcomes (up to 2 years after treatment) for the PACE-C trial.
Materials/Methods:
1208 men with localised prostate cancer (stage T1c-T3a, = Gleason 4+4, PSA = 30ng/mL) were randomised (1:1) to SBRT (36.25 Gy in 5 fractions over 1–2 weeks) or MHRT (60 Gy in 20 fractions over 4 weeks), with 6–12 months of planned ADT. Late toxicity was assessed using RTOG and CTCAE at 6, 9, 12, 18, and 24 months. Co-primary late toxicity endpoints were the incidence of grade 2 or higher (G2+) gastrointestinal (GI) and genitourinary (GU) RTOG toxicities at 2 years. Secondary outcomes were CTCAE incidence and RTOG/CTCAE cumulative incidence (Kaplan-Meier) of G2+ GI/GU toxicities at 2 years, and the proportion of patients with a minimally clinically important difference (MCID) in EPIC-26 urinary incontinence (UI) (8 points), urinary irritative/obstructive (UO) (6 points) and bowel function (5 points) scores at 2 years. Comparisons were by treatment received, with proportions compared by chi-squared test. Significance level was 0.025 for co-primary and 0.01 for other endpoints.
Results:
Baseline characteristics were similar between the SBRT (584 treated / 607 allocated) and MHRT (608 / 601) groups. Median age was 73.1 vs 72.4 years; intermediate-risk disease (NCCN criteria) was present in 65% vs 63%, and high-risk in 35% vs 37%; median PSA was 8.5 ng/mL vs 8.3 ng/mL. Late toxicity data were available for 584 SBRT and 604 MHRT patients. At two years, RTOG G2+ GU toxicity was higher with SBRT vs MHRT (9% (46/536) vs 3% (14/555), p<0.0001), as was CTCAE G2+ GU toxicity (13% (70/544) vs 4% (20/560), p<0.0001). Cumulative RTOG/CTCAE G2+ GU incidence was 24% (135/583) / 32% (184/583) for SBRT and 10% (57/602) / 13% (77/602) for MHRT. GI toxicity at two years was similar between SBRT and MHRT: RTOG G2+ GI toxicity (2% (9/537) vs 2% (11/557), p=0.71), and CTCAE G2+ GI toxicity (3% (19/544) vs 3% (17/560), p=0.67). Cumulative RTOG/CTCAE G2+ GI incidence was 8% (48/582) /13% (75/582) for SBRT and 6% (33/601) / 10% (60/602) for MHRT. G3+ GI and GU toxicities at two years were <2% for both groups. MCID in UO at two years was significantly higher with SBRT vs MHRT (46% (191/418) vs 27% (120/447), p<0.0001), though no significant difference was seen in UI (32% (144/445) vs 25% (117/470), p=0.012) or bowel function (38% (169/447) vs 32% (147/466), p=0.047).
Conclusion:
At two years, bowel toxicity was similar between SBRT and MHRT, while the incidence of urinary toxicity was higher with SBRT, as measured using RTOG, CTCAE and EPIC-26. Five-year toxicity and efficacy outcomes are awaited.
Tata Memorial Centre, Mumbai, India
V. Murthy1, P. Maitre1, M. Pal1, R. Sharma2, L. Pujari3, D. Gudipudi2, D. M. Joseph4, B. Bandekar3, R. Krishnatry1, M. Singh1, P. Verma1, S. Kannan5, R. Phurailatpam6, A. Arora1, A. Joshi1, V. Noronha1, K. Prabhash1, S. Menon1, G. Bakshi1, and G. Prakash1
1Tata Memorial Centre, Homi Bhabha National Institute, Mumbai, India, 2Basavatarakam Indo-American Cancer Hospital and Research Institute, Hyderabad, India, 3Mahamana Pandit Madan Mohan Malaviya Cancer Centre and Homi Bhabha Cancer Hospital, Homi Bhabha National Institute, Varanasi, India, 4All India Institute of Medical Sciences, Dehradun, India, 5ACTREC, Tata Memorial Centre, Homi Bhabha National Institute, Navi Mumbai, India, 6ACTREC, Tata Memorial Centre, Homi Bhabha National Institute, Mumbai, India
Purpose/Objective(s):
To report clinical outcomes from the multicenter phase III randomized trial of adjuvant radiotherapy (RT) after radical cystectomy (RC) and chemotherapy in locally advanced muscle-invasive bladder cancer (LA-MIBC).
Materials/Methods:
Patients with high-risk (T3-4, N1-3, R+) non-metastatic urothelial MIBC post-RC were randomized 1:1 to adjuvant RT or observation (Obs), stratified by nodal stage (N0 vs N+) and chemotherapy (neoadjuvant/adjuvant/none). Cystectomy bed and pelvic nodes were treated with stoma-sparing RT to 50.4Gy in 28 fractions. Primary endpoint of 2-year locoregional failure-free survival (LRFS) and secondary endpoints of bladder cancer-specific survival (BCSS), disease-free survival (DFS), and overall survival (OS) were compared per protocol by log rank test. Competing risk analysis using Fine Gray model compared subdistribution hazard ratios (sHR) for LRFS (competing risks: distant metastases and non-cancer death) and DFS (competing risk: non-cancer death) between the two arms.
Results:
Total 153 patients were randomized from 2016 to 2024 (RT = 77, Obs = 76). Overall, 62% patients had pT3-T4 and 41% had pN+ disease, and a variant histology component in 28% patients. Chemotherapy was neoadjuvant for 71% and adjuvant for 20% patients. No patients received immunotherapy. In RT arm, 63 received planned RT and 14 (defaulted/refused RT = 8, pre-RT progression =4, RT deemed unfeasible = 2) were analyzed with the Obs group (n=90).
Over a median follow-up was 23 months (42 months for survivors), 37% patients had recurred, with 18% locoregional recurrences (RT 8% vs Obs 26%, p=0.006). Two-year LRFS was 65.3% (RT) vs 57.4% (Obs) (HR 0.74, 95% CI 0.46-1.19, p=0.22). Two-year DFS was 59.9% vs 52.8% (HR 0.74, 0.47-1.17, p=0.20), and BCSS was 77.6% vs 64.4% (HR 0.57, 0.31-1.07, p=0.07) respectively. RT showed significantly better LRFS (sHR 0.55, 0.31-0.97, p=0.04) and DFS (sHR 0.55, 0.32-0.95, p=0.03) in competing risk analysis. Overall, 45% patients died (31% due to disease, 14% other cause). Two-year OS was 68.1% (RT) vs 57.0% (Obs) (HR 0.80, 0.49-1.30, p=0.4). There were no isolated locoregional recurrences in the RT arm, with 2-year locoregional control 91.2% (RT) vs 76.4% (Obs) (HR 0.27, 0.10-0.71, p=0.004). Subgroup analysis showed significant benefit with RT in T3-T4 (sHR LRFS 0.40, DFS 0.42) and N+ disease (sHR LRFS 0.39, DFS 0.40). Late grade 3+ toxicity was similar (RT 8.5% RT vs Obs 10.5%, p=0.6).
Conclusion:
Adjuvant RT improved LRFS and DFS without increased severe late toxicity in patients with LA-MIBC post cystectomy and chemotherapy. Potential benefits in OS is being explored in a planned individual patient data meta-analysis of randomized trials.
Table 1: Patterns of failure
(* with synchronous distant metastases)
Total | Obs | RT | p | |
Cystectomy bed | 8.5% | 13.3% | 1.6%* | 0.01 |
Regional | 15.7% | 21.1% | 7.9%* | 0.03 |
Distant | 29.4% | 28.9% | 30.2% | 0.87 |
Unknown | 0.6% | 1.1% | 0% |
Tata Memorial Centre, Mumbai, India

Queen Elizabeth Hospital, Birmingham, United Kingdom
Timothy Jackson, Jenny Sherriff, Talha Maqsood
Radiotherapy, Queen Elizabeth Hospital, Birmingham, United Kingdom
Purpose/Objective:
Recent publications[1][2] have suggested spinal cord constraints for spinal cord Stereotactic Ablative Body Radiotherapy (SABR), lower than has previously been published such as in TG101 [3]. Within the UK there is increasing interest in spinal SABR. To date the majority of published studies considering spinal SABR toxicity are limited by small numbers of patients. The 2022 dose consensus[1] discusses 7 studies in the literature, with 2 over 100 patients, but includes 4 less than 30 patients.
The presented series includes 130 treatments of 119 patients, with a minimum of 18 months follow up. This is a valuable addition to the literature due to the precise treatment on the Cyberknife platform, high resolution pre treatment imaging, and intrafraction target tracking ensuring dose reported is known accurately. The significant number of patients treated and quality of follow up allows confidence in conclusions drawn.
Material/Methods:
All structures were contoured using CT, t1 VIBE and t2 SPACE MRI scans with 1mm resolution, according to UK SABR consortium guidelines. The target is at minimum the full vertebral body. Plan prescription dose range was 24 – 27Gy in 3 fractions and TG101 tolerances used. Mean PTV volume was 56.8cc. Cord was grown by 2mm isotropically to create CordPRV. During treatment delivery, CyberKnife spine tracking had an end-to-end accuracy averaging 0.7mm for these patients. Images were taken and live treatment correction was applied every 30-45 seconds throughout treatment.
Plan dose information was recorded. Patient hospital clinic appointments and GP records were checked for toxicity and this was recorded. A minimum of 18 months follow up was required.
Results:
10 patients died prior to 18 months after treatment or were lost to follow up, with none reporting myelopathy. 109 patients had records from phone clinic, hospital clinic attendance, or GP records where patients were assessed. No cases of myelopathy were recorded. In 49/130 patient treatments, CordPRV dose was above recent tolerance 2022 dose consensus tolerance [1] but below TG101 tolerance [3]. In 109/130 patient treatments, the spinal canal was above 22Gy(0.1cc), and within [1] and [3] 24Gy tolerance.
Conclusion:
130 spinal treatments were planned above recent tolerances with 5% risk of myelopathy [1] and delivered with no myelopathy seen. Given the low number of spinal patient series in the literature, and the high resolution, precise treatment, and intrafraction tracking for these patients, this is very valuable for understanding safe doses for treatment near the spinal cord.

Stanford University School of Medicine, Palo Alto, USA
David J. Park, Isabelle Lee, Shreyas Annagiri, Kuan-Nien Chou, Aroosa Zamarud, Deyaaldeen Abu reesh, Amirhossein Akhavan-Sigari, Yusuke S. Hori, Amit Persad, Fred Lam, Xuejun Gu, Erqi Pollom, Steven D. Chang
Neurosurgery, Stanford University School of Medicine, Palo Alto, USA
Objectives:
Spinal metastases (SM) with epidural spinal cord compression (ESCC) present a significant challenge due to the high risk of radiation-induced injury to critical structures such as the spinal cord and nerve roots. Traditional treatment approaches often avoid circumferential stereotactic body radiotherapy (SBRT) to reduce these risks. The efficacy and safety of donut-shaped circumferential SBRT, designed to target the spinal column while sparing the spinal cord, remains underexplored. This study aims to evaluate the safety and efficacy of donut-shaped circumferential CyberKnife SBRT for spinal metastases, particularly in preventing radiation-induced myelopathy and achieving local tumor control.
Methods:
We retrospectively analyzed data from patients treated with donut-shaped circumferential SBRT between 2014 and 2023. Key parameters examined included patient demographics, ESCC grade (Bilsky), prior treatments, clinical symptoms, and treatment parameters. We focused on SBRT dosimetric data, radiation exposure to the spinal cord and cauda equina, adherence to dose-volume constraints, and post-SBRT outcomes, including myelopathy and local tumor control.
Results:
Forty-eight lesions in 43 patients (median age: 65; range: 20-78) were reviewed. One patient required separation surgery for severe ESCC (Bilsky grade 3). The median clinical target volume (CTV) was 63.77 cm³, and the median margin dose was 24 Gy. Over a median follow-up of 8 months, local tumor control was 91.1% at 6 months, 87.1% at 1 year, 82.8% at 3 years, and 62.1% at 5 years. Median overall survival was 17 months. Of the 21 lesions exceeding dose constraints, only one patient exhibited clinical myelopathy, which correlated with local tumor recurrence. No radiographic myelopathy or other radiation-induced complications were observed.
Conclusion(s):
Donut-shaped circumferential CyberKnife SBRT is a safe and effective treatment for spinal metastases, achieving high local tumor control with minimal radiation-induced complications, including myelopathy.

McMaster University – Juravinski Cancer Centre, Hamilton, ON, Canada
E. Donovan1,2, K. L. Schnarr3, J. N. Greenspoon4, J. Wright5, C. Hann6, A. C. Whitton5, T. Chow5, Y. Wang7, S. Parpia1, T. J. Whelan4, and A. Swaminath8
1McMaster University – Juravinski Cancer Centre, Hamilton, ON, Canada, 2Department of Radiation Oncology, McMaster University, Hamilton, ON, Canada, 3Division of Radiation Oncology, Juravinski Cancer Centre, Hamilton, ON, Canada, 4McMaster University, Hamilton, ON, Canada, 5Juravinski Cancer Centre, Hamilton, ON, Canada, 6Juravinski Cancer Centre-McMaster University, Hamilton, ON, Canada, 7McMaster, Hamilton, ON, Canada, 8Juravinski Cancer Centre, McMaster University, Hamilton, ON, Canada
Purpose/Objective(s):
Metastatic epidural spinal cord compression (MESCC) is a devastating complication of advanced malignancy resulting in significant functional deterioration. Palliative 3D-conformal radiotherapy (3DCRT) is the standard treatment in non-surgical candidates, but pain, motor and neurologic outcomes are variable. We conducted a pilot study to determine if a stereotactic body radiotherapy (SBRT) boost in addition to 3DCRT would be feasible, and what effects this would have on toxicity and functional outcomes.
Materials/Methods:
Eligible patients included those with a solid malignancy, evidence of at least Bilsky 1c MESCC, and Rades motor scale function of at least 3. Patients were initially treated with 3DCRT (either 20 Gy/5 fractions or 8 Gy/1 fraction). SBRT boost was delivered within 4-6 weeks following 3DCRT, using a robotic radiosurgery technique, to a dose of 18-24 Gy/2 fractions. The primary outcome was feasibility of planning and delivery of 3D CRT and SBRT boost, with a success rate defined as 80% of accrued patients (95% confidence interval 75-97%). Secondary endpoints included changes in motor and ambulatory function, pain control (using Brief Pain Inventory), toxicity, as well as quality of life (QoL) measured using EORTC QLQ-c30 and BM22 questionnaires. Planned sample size was 30 patients.
Results:
Sixteen patients were initially accrued from 2018-2023, the trial closed to slow accrual due to COVID-19. 13 patients were treated successfully with SBRT boost following 3DCRT, meeting the primary outcome (0.81, 0.57-0.93). Median baseline motor score was 7 normal (range 2-7), pain score was 5.5 (1-10), and most patients were ambulatory. Most had a solitary spinal site of metastasis (53.3%), and Bilsky 1c or 2 MESCC (66.7%). A majority received 20 Gy/5 fraction 3DCRT (81.3%), and SBRT boost was given a median of 36 days afterwards (33-50.1 IQR). Motor function was maintained in 76.9% and improved by 2 points from baseline in 15.4% of patients at 1-month post-SBRT boost and was subsequently maintained in patients at 3 and 6 months. Ambulatory function improved in 15.4% and was maintained in 69.2% of patients at 1 month, and improved again at 3- and 6-months post SBRT in 18.2% and 12.5% respectively. Pain improved in 23.1%, 18.2% and 37.5% of patients at 1, 3 and 12 months respectively. Only 1 Grade 3 toxicity (chest wall pain) occurred which resolved at 3 months. Median global QoL improved from baseline (69.2), to 76.3, 76.6 and 82.5 at 1,3 and 6 months respectively. BM 22 scores improved in functional and pain domains at 1,3, and 6 months. There were 2 local recurrences (143 and 236 days), and median survival of the entire cohort was 8.9 months (7.8-NR)
Conclusion:
SBRT boost following 3DCRT for MESCC was feasible, with no added neurological toxicity, and resulted in moderate improvements or prolonged maintenance of motor and ambulatory function, and pain control. QoL tended to improve over time from treatment. This regimen may provide additional benefit for select MESCC patients.

H. U. Ramón y Cajal, Madrid, Spain
Adrián Durango Méndez1, David Sevillano Martínez2, Maria E Centelles Hidalgo1, Juan D Garcia Fuentes2, Ignacio M Gomez Paloma1, Margarita Martin Martin1, Mercedes Martin Sanchez1, Isabel Alvira Ortiz1, Maria D Espinosa Cuesta1, Carolina De La Pinta Alonso1, Eva Fernandez Lizarbe1, Feliciano Garcia Vicente2, Sonsoles Sancho Garcia1
1 2Radiotherapy Oncology, H. U. Ramón y Cajal, Madrid, Spain. Physics, H. U. Ramón y Cajal, Madrid, Spain
Purpose/Objective:
To evaluate the efficacy and safety of stereotactic body radiotherapy (SBRT) using the CyberKnife system for spine metastases, focusing on patient outcomes, progression-free survival (PFS), and treatment-related toxicities.
Material/Methods:
From May 2004 to August 2024, 61 patients with 73 spine metastases were treated using Robotic Radiosurgery Unit CyberKnife in our centre. The mean age at diagnosis was 61 years. Baseline performance status showed 94% of patients with an ECOG score of 1–2 and 74.6% with a Karnofsky index of 90 or higher. Patient eligibility for spine SBRT was determined based on the SINS scale and Bilsky classification. Treatment doses varied from single-fraction regimens in which the most frequent dose was 18Gy, to multi-session regimens of 21-35Gy in 3-5 fractions. The mean planning target volume (PTV) was 53.47 cc, with a mean maximum dose in PTV of 22,8Gy for single fraction; 29.5Gy for 3 fractions schemes and 32.13Gy for 5 fractions schemes.
Results:
The median follow-up was 21 months (1-60). Local control at 24 months for patients receiving single-fraction SBRT was 92.1% compared to 88% for those treated with fractionated schemes. The median progression-free survival has not been reached. At two years local relapse free survival was 90%.
Median overall survival was 40 months. The two-year overall survival was 65.4%. There was no significant difference in overall survival between the different fractionation regimens.
Regarding tolerance, 89.6% of patients experienced no acute toxicities from SBRT. Seven patients reported acute toxicity, none exceeding grade II. The most common acute side effects included asthenia followed by esophagitis and enteritis.
6 cases of vertebral compression fracture (VCF) have been reported out of 73 lesions treated (8.22%). All cases of VCFs occurred in patients treated with a single fraction. There are no significant differences in the maximum dose in PTV or in the degree of previous SINS related to the VCFs cases.
Conclusion:
These findings support CyberKnife-based SBRT as an effective and safe modality for managing spine metastases. While single-fraction regimens may provide higher local control, it also carries a higher risk of VCF, highlighting the need for careful patient selection. Future studies should focus on refining dosing strategies to optimize efficacy and minimize adverse effects.

Erasmus MC Cancer Institute, University Medical Center, Rotterdam, Netherlands
Lucy A. van Werkhoven, Maaike T.W. Milder, Mischa S. Hoogeman, Remi A. Nout, Joost J. Nuyttens
Radiotherapy, Erasmus MC Cancer Institute, University Medical Center, Rotterdam, Netherlands
Purpose/Objective:
We report dosimetric outcomes of a phase-II study in patients undergoing CT-guided, radiotherapy technologist (RTT) only, online adaptive stereotactic body radiotherapy (SBRT) on abdominal and pelvic lymph node oligometastases (A-P LN), to assess if this approach can iso-toxically increase the target dose.
Material/Methods:
Patients with oligometastatic A-P LN received 45 Gy in five fractions on the CyberKnife in the phase-II trial. For each patient, three plans were created using pre-treatment CT scans: Plan A, Standard of care (SOC) plan based on the planning CT prescribed to the 90% isodose-line; Plan B, adaptive plan with organ at risk (OAR) contours from a diagnostic CT and prescribed to the 90% isodose-line; Plan C, an adaptive plan, based on the planning CT prescribed to the 80% isodose-line. After a pre-fraction in-room CT scan on rails [1], the RTT used a decision tree to select the plan with the highest target coverage without exceeding OAR constraints (Figure 1). Dose volume histogram (DVH) parameters of the target and OAR were extracted from planning and fraction CTs to determine if the adaptive treatment increased the target dose without increasing dose to the OAR.
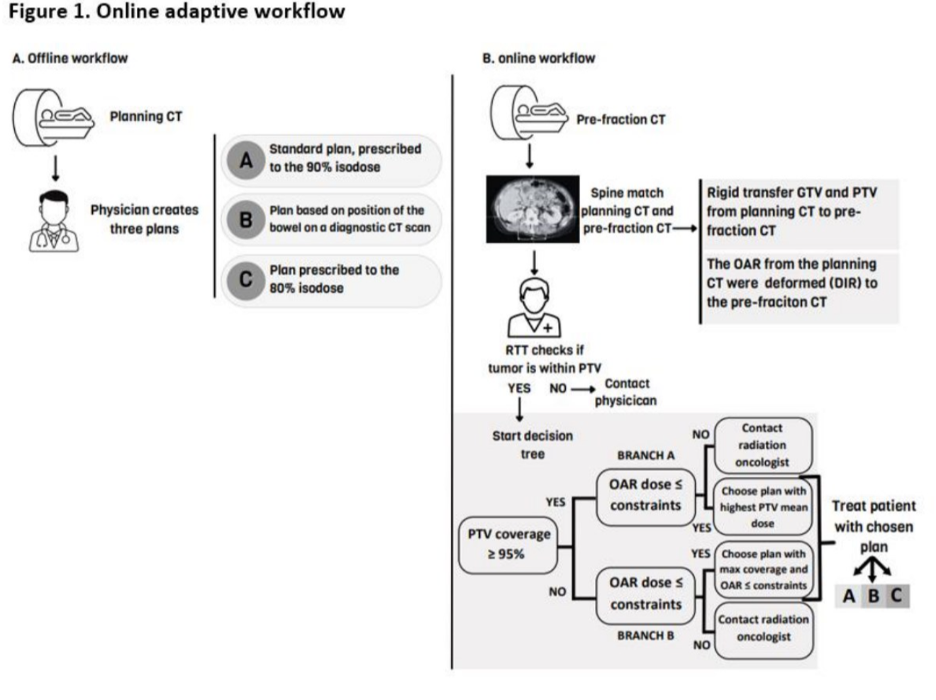
Results:
In total, 52 patients were included, and 55 online adaptive treatments were performed. An adaptive plan was chosen in 58% of fractions and 78% of patients were treated with at least one adaptive plan. This resulted in a significantly higher given GTV Dmean compared to the planned dose (100.6 BED10 vs. 95 BED10, P< 0.001). The dose to D0.5cc of the gastro-intestinal organs (GIO) was 2.3 Gy EQD2 higher for the SOC plan on the fraction CT compared to the SOC plan on the original planning CT (P=0.009), this finding represents the dosimetric impact of inter-fraction motion without plan adaption. The GIO D0.5cc was also 2.7 Gy EQD2 higher (p=0.01) on the fraction CT with the given plan compared to the SOC plan on the planning CT scan. However, no significant difference in GIO D0.5cc was found between the SOC plan on the fraction CT and the given plan on the fraction CT: this increased dose is not an effect of plan adaption.
Conclusion:
With an RTT-only, CT-based online adaptive SBRT workflow for A-P LN oligometastases, using a library of plans, 78% of the patients was treated with adaptive radiotherapy. This workflow enabled an iso-toxically delivered mean GTV BED10 5 Gy dose increase and offers a chance of better oncological outcomes.

ARNAS Civico Hospital, Palermo, Italy
F. Cuccia1, M. Campione2,3, S. D’alessandro1, G. Mortellaro1, A. Spera1, V. Figlia1, G. Musicò4, A. Abbate4, S. Russo5, C. Messina5, G. Carruba2, L. Blasi5, and G. Ferrera1
1Radiation Oncology – ARNAS Civico Hospital, Palermo, Italy, 2Clinical Research – ARNAS Civico Hospital, Palermo, Italy, 3Kore University, Enna, Italy, 4Gynecology Oncology – ARNAS Civico Hospital, Palermo, Italy, 5Medical Oncology – ARNAS Civico Hospital, Palermo, Italy
Purpose/Objective(s):
Peritoneal carcinosis can occur in several gastrointestinal or gynecological malignancies and its prognosis is usually poor. With the advent of more effective systemic agents, the overall survival of metastatic patients has been revolutionized and isolated peritoneal or abdominal wall metastases might benefit from local treatments. Traditionally the role of radiotherapy for this challenging scenario was limited to palliative intent with modest results, but Stereotactic Body Radiotherapy (SBRT) might be considered in selected patients with oligometastatic presentation.
Materials/Methods:
The present study collects the outcomes of a total of 26 lesions in 20 patients who received SBRT to oligometastatic disease located in the peritoneum or in the abdomino-pelvic wall. Oligometastases were defined according to recent ESTRO/EORTC consensus. Inclusion criteria were as follows: ECOG PS=2, written informed consent, up to 5 lesions to be treated at the same time, patients treated with radiotherapy schedules applying minimum 6 Gy per fraction. Primary endpoint of the study was local control (LC); acute and late toxicity, distant progression-free survival (DPFS), time-to-next systemic treatment (TNST), polymetastatic-free survival (PMFS) and overall survival (OS) were secondary endpoints. Toxicity was assessed according to CTCAE criteria v5.0. Survival estimates were performed using Kaplan-Meier method, uni- and multi-variate analyses were carried out to identify any potentially significant correlation.
Results:
Between April 2020 and September 2024 a total of 26 oligometastatic lesions located in the peritoneum or in the abdominal wall detected in 20 patients received SBRT with Helical TomoTherapy. All cases have been assessed in multidisciplinary team. Only in three patients out of 20, more than one lesion received SBRT: 2 lesions in 2 patients, and five lesions in a single case of colorectal cancer with ongoing 3rd line systemic treatment. Median total dose was 30 Gy (27-35 Gy) in 5 fractions (3-5). The most frequent primary neoplasm was ovarian cancer in 14/20, endometrial in 2/20, while the remaining were colorectal, vaginal, pancreatic and non-small cell lung cancer. Four lesions were located in the abdominal wall, while the remaining 22 in the peritoneum. Concurrent systemic therapy was administered in 18/20 patients. With a median follow-up of 15 months (range, 6-59), our 1-year LC was 100%, while 1-year DPFS, PMFS, TNTS and OS rates were 54%, 69%, 61% and 83%, respectively. At statistical analysis, abdominal wall lesions were significantly related to improved OS rates (p=0.03), as well as patients who developed a further oligometastatic progression treated with a second course of SBRT (p=0.04). No G=3 adverse events occurred.
Conclusion:
Our preliminary data support the use of SBRT in selected cases of oligometastatic disease located in the peritoneum or in the abdominal wall with excellent results in terms of tolerability and promising clinical outcomes.

IRCCS San Raffaele, Milan, Italy
Gaia Parma1, Sara Saufi1, Andrei Fodor1, Chiara L Deantoni1, Fiorino Claudio2, Antonella Del Vecchio2, Stefano Arcangeli3,4, Nadia G Di Muzio1,5
1 2 3 Radiotherapy, IRCCS San Raffaele, Milan, Italy. Medical Physics, IRCCS San Raffaele, Milan, Italy. Radiotherapy, IRCCS San Gerardo dei Tintori, Monza, Italy. 4Radiotherapy, Università degli Studi Milano Bicocca, Monza, Italy. 5 Radiotherapy, Vita-Salute San Raffaele University, Milan, Italy
Purpose/Objective:
MITO multicenter retrospective trials demonstrated the significant role that radiotherapy (RT) can play in oligometastatic gynecological cancers (1,2,3). In this retrospective study we analyzed outcomes and safety of robotic stereotactic body radiotherapy (SBRT) performed in our institution for the oligometastatic disease from gynecological tumors.
Material/Methods:
From January 2018 to August 2024 a total of 99 oligometastases were treated in 54 patients with gynecological cancer with robotic SBRT (CyberKnife®, Accuray, Sunnyvale CA, USA). Median prescribed dose was 40 (18-60) Gy in a median of 5 (1-8) fractions, at a median isodose of 79.0% (67-83%). Oligometastatic lesions were localized in: lymph nodes in 38.4% of cases, lung in 37.4%, liver in 8.1%, bone in 7.1%, brain in 6%, and other sites in 3% of cases.
Endometrial cancer was the most common primary tumor (63% of patients). Median GTV was 2.58cc. Median age at treatment was 67 years (22-91). Toxicity was assessed using CTCAE v 5.0 criteria. The primary endpoint was the complete response rate to SBRT. The secondary aims were local relapse-free survival (LRFS), disease-free survival (DFS), overall survival (OS), as well as toxicity.
Results:
Median follow-up was 36 months. Grade (G)1 and 2 acute toxicity was observed in 8.1% of patients. No G≥3 acute toxicity was observed. Late toxicity was low, only 5% of patients presented a G1 toxicity. Complete response was found in 61.6% of lesions (only 5% of patients did not respond to SBRT). Twelve- month LRFS and DFS were 89.4% and 37%; at 24 and 36 months LRFS and DFS were 87.9% and 19.9%, respectively (Fig. 1). OS was 81.5% at 12 months, 68% at 24 months and 19.9% at 36 months.
The 1- and 2 year actuarial DFS rate were 42% and 23% in patients with complete response versus 23% and 9% in patients with partial response, stable, or progressive disease (p=0.005) (Fig.2).
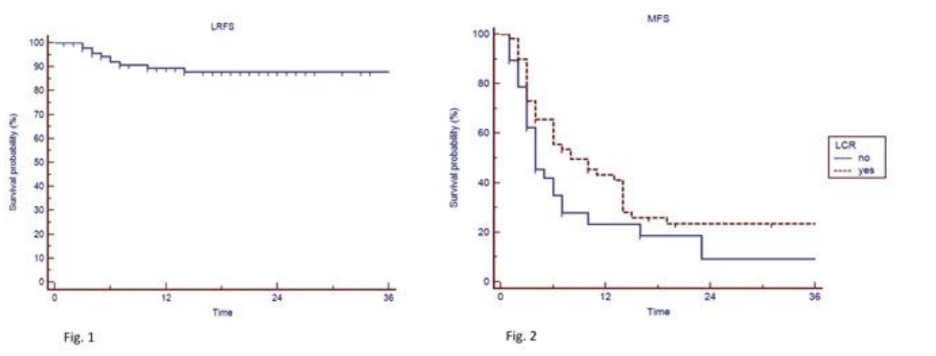
Conclusion:
In our experience, using higher median doses than in the MITO retrospective trials, we observed high rate of local complete response and persistent long term LRFS. Patients with complete response after SBRT had a statistically significant higher rate of DFS, than those with partial/ stable response or progressive disease, thus demonstrating that local control in oligometastatic patients from gynecological cancers is a relevant objective. Prospective studies are needed to confirm these results.
European Institute of Oncology, Milan, Italy